## Diagram: Medical Pathophysiology Flowchart
### Overview
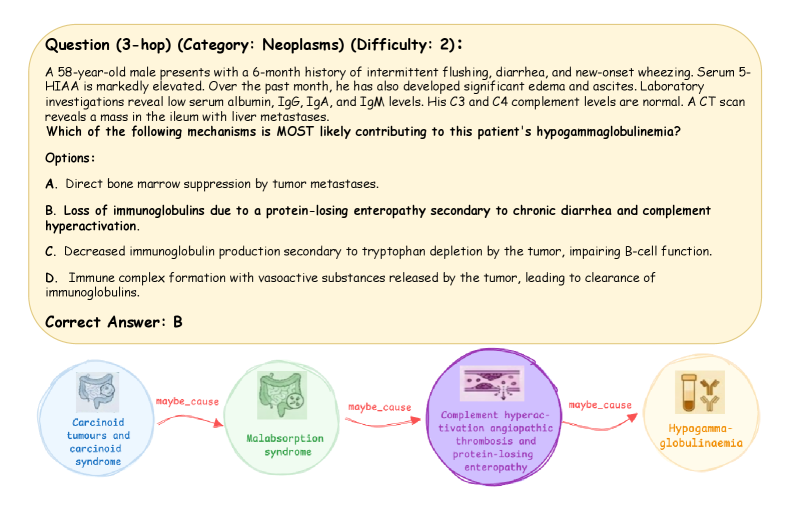
The image contains a medical question (3-hop, Category: Neoplasms, Difficulty: 2) followed by a flowchart illustrating a causal chain of medical conditions. The flowchart connects four medical syndromes via "maybe_cause" arrows, ending with hypogammaglobulinemia.
### Components/Axes
1. **Question Text**:
- Patient case: 58-year-old male with 6-month history of flushing, diarrhea, wheezing, elevated 5-HIAA, low serum albumin/IgG/IgA/IgM, normal C3/C4, ileal mass with liver metastases.
- Question: Which mechanism most likely contributes to hypogammaglobulinemia?
- Options:
- A. Direct bone marrow suppression by tumor metastases.
- B. Loss of immunoglobulins due to protein-losing enteropathy secondary to chronic diarrhea and complement hyperactivation.
- C. Decreased immunoglobulin production secondary to tryptophan depletion by the tumor, impairing B-cell function.
- D. Immune complex formation with vasoactive substances released by the tumor, leading to immunoglobulin clearance.
- Correct Answer: B
2. **Flowchart**:
- **Nodes**:
1. **Carcinoid tumours and carcinoid syndrome** (blue circle, leftmost).
2. **Malabsorption syndrome** (green circle, center-left).
3. **Complement hyperactivation angioedema protein-losing enteropathy** (purple circle, center-right).
4. **Hypogammaglobulinemia** (orange circle, rightmost).
- **Arrows**:
- All arrows labeled "maybe_cause" (red text).
- Flow direction: Carcinoid tumors → Malabsorption syndrome → Complement hyperactivation → Hypogammaglobulinemia.
### Detailed Analysis
- **Flowchart Connections**:
- Carcinoid tumors (neuroendocrine tumors) are linked to carcinoid syndrome (flushing, diarrhea, wheezing via serotonin release).
- Malabsorption syndrome (green node) is proposed as a secondary effect, potentially due to intestinal damage from tumor metastases.
- Complement hyperactivation (purple node) is tied to angioedema and protein-losing enteropathy, which aligns with the patient’s low serum albumin and immunoglobulins.
- Hypogammaglobulinemia (orange node) is the final outcome, explained by chronic protein loss and complement-driven immunoglobulin depletion.
- **Textual Labels**:
- All flowchart nodes and arrows are explicitly labeled. No numerical data or scales are present.
### Key Observations
- The flowchart emphasizes a **causal chain** starting with carcinoid tumors and ending with hypogammaglobulinemia.
- The correct answer (B) directly references **protein-losing enteropathy** and **complement hyperactivation**, which are central to the flowchart’s final node.
- Option C (tryptophan depletion) and D (immune complex formation) are not reflected in the flowchart, suggesting they are distractors.
### Interpretation
The flowchart illustrates a plausible pathophysiological pathway for hypogammaglobulinemia in this patient:
1. **Carcinoid tumors** cause carcinoid syndrome (symptoms match the case).
2. **Malabsorption syndrome** (likely from intestinal metastases) leads to **protein-losing enteropathy**, reducing serum albumin and immunoglobulins.
3. **Complement hyperactivation** (from chronic inflammation) exacerbates protein loss, further depleting immunoglobulins.
4. **Hypogammaglobulinemia** results from sustained protein loss and immune dysregulation.
This aligns with the patient’s lab findings (low IgG/IgA/IgM, normal complement levels) and supports **Answer B** as the most likely mechanism. The flowchart visually reinforces the connection between tumor-related diarrhea, protein loss, and immunodeficiency.