## Clinical Note to Diagnosis Flow Diagram
### Overview
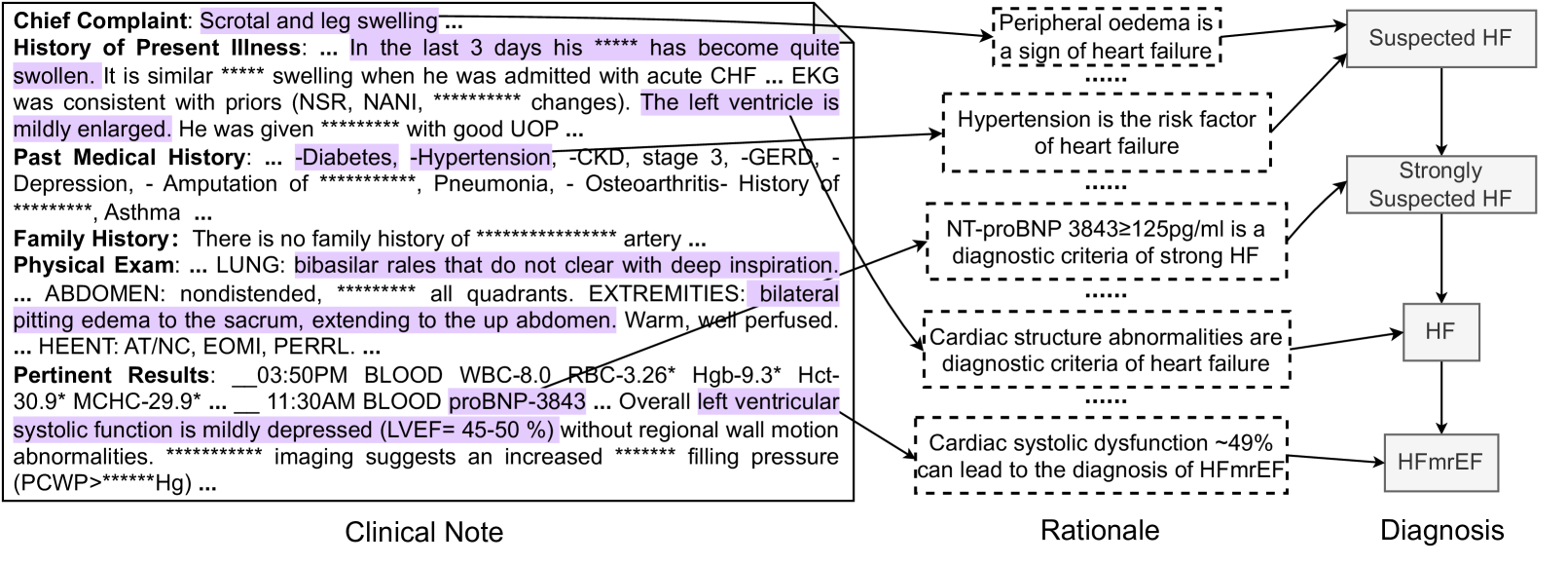
The image presents a flow diagram that connects clinical observations from a patient's medical history and physical exam to a final diagnosis of HFmrEF (Heart Failure with mid-range Ejection Fraction). The diagram links information from a "Clinical Note" to a "Rationale" section, ultimately leading to a "Diagnosis."
### Components/Axes
* **Clinical Note:** This section contains information gathered from the patient's chief complaint, history of present illness, past medical history, family history, physical exam, and pertinent results.
* **Rationale:** This section provides the reasoning and medical knowledge that connects the clinical findings to the diagnosis.
* **Diagnosis:** This section presents the final diagnosis based on the clinical note and rationale. The diagnoses are: Suspected HF, Strongly Suspected HF, HF, and HFmrEF.
### Detailed Analysis or ### Content Details
**Clinical Note:**
* **Chief Complaint:** Scrotal and leg swelling.
* **History of Present Illness:** In the last 3 days, the patient's condition has become quite swollen. The swelling is similar to when the patient was admitted with acute CHF. EKG was consistent with priors (NSR, NANI, changes). The left ventricle is mildly enlarged. The patient was given with good UOP.
* **Past Medical History:** Diabetes, Hypertension, CKD (stage 3), GERD, Depression, Amputation, Pneumonia, Osteoarthritis, History of Asthma.
* **Family History:** There is no family history of artery.
* **Physical Exam:**
* LUNG: Bibasilar rales that do not clear with deep inspiration.
* ABDOMEN: Nondistended, all quadrants.
* EXTREMITIES: Bilateral pitting edema to the sacrum, extending to the up abdomen. Warm, well perfused.
* HEENT: AT/NC, EOMI, PERRL.
* **Pertinent Results:**
* 03:50 PM BLOOD: WBC-8.0, RBC-3.26*, Hgb-9.3*, Hct-30.9*, MCHC-29.9*.
* 11:30 AM BLOOD: proBNP-3843. Overall left ventricular systolic function is mildly depressed (LVEF = 45-50%) without regional wall motion abnormalities. Imaging suggests an increased filling pressure (PCWP > Hg).
**Rationale:**
* Peripheral oedema is a sign of heart failure.
* Hypertension is the risk factor of heart failure.
* NT-proBNP 3843 ≥ 125 pg/ml is a diagnostic criteria of strong HF.
* Cardiac structure abnormalities are diagnostic criteria of heart failure.
* Cardiac systolic dysfunction ~49% can lead to the diagnosis of HFmrEF.
**Diagnosis:**
* Suspected HF
* Strongly Suspected HF
* HF
* HFmrEF
### Key Observations
* The diagram illustrates a step-by-step process of how clinical information is used to arrive at a diagnosis of HFmrEF.
* The rationale section provides the medical justification for each diagnostic step.
* The clinical note contains a mix of subjective (patient complaints) and objective (lab results, physical exam findings) data.
* The proBNP value of 3843 is significantly higher than 125 pg/ml, supporting the diagnosis of strong HF.
* The LVEF of 45-50% falls within the range for HFmrEF.
### Interpretation
The diagram effectively demonstrates the clinical reasoning process involved in diagnosing heart failure. It highlights the importance of integrating patient history, physical exam findings, and laboratory results to arrive at an accurate diagnosis. The flow from "Clinical Note" to "Rationale" to "Diagnosis" provides a clear and logical framework for understanding the diagnostic process. The diagram emphasizes the role of specific clinical findings, such as peripheral edema, hypertension, elevated proBNP, and reduced LVEF, in supporting the diagnosis of HFmrEF. The diagram suggests a systematic approach to diagnosis, where each piece of evidence contributes to the final conclusion.