# DiReCT: Diagnostic Reasoning for Clinical Notes via Large Language Models
**Authors**: {, , }, , {, , }
## Abstract
Large language models (LLMs) have recently showcased remarkable capabilities, spanning a wide range of tasks and applications, including those in the medical domain. Models like GPT-4 excel in medical question answering but may face challenges in the lack of interpretability when handling complex tasks in real clinical settings. We thus introduce the diagnostic reasoning dataset for clinical notes (DiReCT), aiming at evaluating the reasoning ability and interpretability of LLMs compared to human doctors. It contains 511 clinical notes, each meticulously annotated by physicians, detailing the diagnostic reasoning process from observations in a clinical note to the final diagnosis. Additionally, a diagnostic knowledge graph is provided to offer essential knowledge for reasoning, which may not be covered in the training data of existing LLMs. Evaluations of leading LLMs on DiReCT bring out a significant gap between their reasoning ability and that of human doctors, highlighting the critical need for models that can reason effectively in real-world clinical scenarios Code are available https://github.com/wbw520/DiReCT. Data will be released through PhysioNet..
footnotetext: Corresponding author.
## 1 Introduction
Recent advancements of large language models (LLMs) [Zhao et al., 2023] have ushered in new possibilities and challenges for a wide range of natural language processing (NLP) tasks [Min et al., 2023]. In the medical domain, these models have demonstrated remarkable prowess [Anil et al., 2023, Han et al., 2023], particularly in medical question answering (QA) [Jin et al., 2021]. Leading-edge models, such as GPT-4 [OpenAI, 2023a], exhibit profound proficiency in understanding and generating text [Bubeck et al., 2023], even achieved high scores on the United States Medical Licensing Examination (USMLE) questions [Nori et al., 2023].
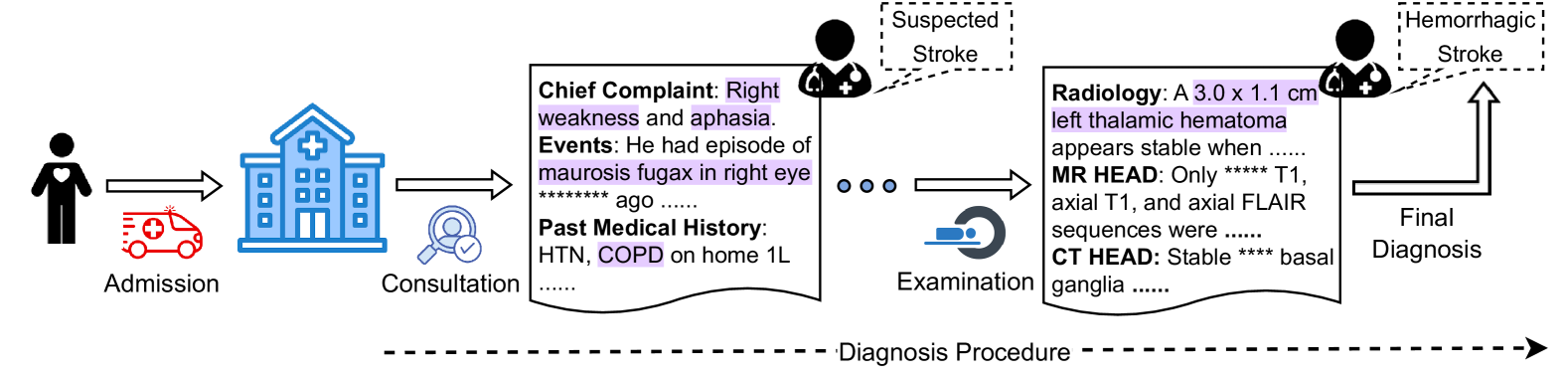
Despite the advancements, interpretability is critical, particularly in medical NLP tasks [Liévin et al., 2024]. Some studies assess this capability over medical QA [Pal et al., 2022, Li et al., 2023, Chen et al., 2024] or natural language inference (NLI) [Jullien et al., 2023]. Putting more attention on interpretability, they use relatively simple tasks as testbeds, taking short text as input. However, tasks in real clinical settings can be more complex [Gao et al., 2023a]. As shown in Figure 1, a typical diagnosis requires comprehending and combining various information, such as health records, physical examinations, and laboratory tests, for further reasoning of possible diseases in a step-by-step manner following the established guidelines. This observation suggests that both perception, or reading, (e.g., finding necessary information in medical record) and reasoning (determining the disease based on the observations) should be counted when evaluating interpretability in LLM-based medical NLP tasks.
For a more comprehensive evaluation of LLMs for supporting diagnosis in a more realistic setting, we propose a Di agnostic Re asoning dataset for C linical no T es (DiReCT). The task basically is predicting the diagnosis from a clinical note of a patient, which is a collection of various medical records, written in natural language. Our dataset contains 511 clinical notes spanning 25 disease categories, sampled from a publicly available database, MIMIC-IV [Johnson et al., 2023]. Each clinical note undergoes fine-grained annotation by professional physicians. The annotators (i.e., the physicians) are responsible for identifying the text, or the observation, in the note that leads to a certain diagnosis, as well as the explanation. The dataset also provides a diagnostic knowledge graph based on existing diagnostic guidelines to facilitate more consistent annotations and to supply a model with essential knowledge for reasoning that might not be encompassed in its training data.
To underscore the challenge offered by our dataset, we evaluate a simple AI-agent based baseline [Xi et al., 2023, Tang et al., 2023] that utilizes the knowledge graph to decompose the diagnosis into a sequence of diagnoses from a smaller number of observations. Our experimental findings indicate that current state-of-the-art LLMs still fall short of aligning well with human doctors.
Contribution. DiReCT offers a new challenge in diagnosis from a complex clinical note with explicit knowledge of established guidelines. This challenge aligns with a realistic medical scenario that doctors are experiencing. In the application aspect, the dataset facilitates the development of a model to support doctors in diagnosis, which is error-prone [Middleton et al., 2013, Liu et al., 2022]. From the technical aspect, the dataset can benchmark models’ ability to read long text and find necessary observations for multi-evidence entailment tree reasoning. As shown in Figure 3, this is not trivial because of the variations in writing; superficial matching does not help, and medical knowledge is vital. Meanwhile, reasoning itself is facilitated by the knowledge graph. The model does not necessarily have the knowledge of diagnostic guidelines. With this choice, the knowledge graph explains the reasoning process, which is also beneficial when deploying such a diagnosis assistant system in practical uses.
<details>
<summary>x1.png Details</summary>
### Visual Description
\n
## Diagram: Stroke Diagnosis Procedure
### Overview
This diagram illustrates the procedure for diagnosing a stroke, starting from patient admission and culminating in a final diagnosis. It depicts a sequential flow of events, including patient presentation, consultation, examination, and radiological findings. The diagram uses icons to represent stages and text boxes to provide details.
### Components/Axes
The diagram is structured horizontally, with stages labeled as:
* **Admission:** Represented by a person icon.
* **Consultation:** Represented by a hospital building icon and a doctor with a stethoscope icon.
* **Examination:** Represented by an eye icon.
* **Final Diagnosis:** Represented by a brain icon.
A dashed line labeled "Diagnosis Procedure" runs horizontally across the bottom, indicating the flow of the process. Text boxes are positioned above each stage, providing details. Dotted lines with rounded rectangles indicate potential diagnoses at intermediate stages.
### Detailed Analysis or Content Details
1. **Admission:**
* No specific data points, but the stage is labeled "Admission".
2. **Consultation:**
* **Chief Complaint:** Right weakness and aphasia.
* **Events:** He had an episode of *maurosis fugax* in right eye ago. (The exact time "ago" is obscured by asterisks).
* **Past Medical History:** HTN, COPD on home 1L (likely referring to 1 liter of oxygen).
3. **Suspected Stroke (Intermediate Diagnosis):**
* Labeled as "Suspected Stroke" within a dotted rounded rectangle.
4. **Examination:**
* **Radiology:** A 3.0 x 1.1 cm left thalamic hematoma appears stable when…
* **MR HEAD:** Only T1, axial T1, and axial FLAIR sequences were…
* **CT HEAD:** Stable basal ganglia…
5. **Hemorrhagic Stroke (Final Diagnosis):**
* Labeled as "Hemorrhagic Stroke" within a dotted rounded rectangle.
6. **Diagnosis Procedure:**
* The dashed line at the bottom is labeled "Diagnosis Procedure".
### Key Observations
* The diagram shows a clear progression from initial symptoms to a final diagnosis.
* The size of the left thalamic hematoma is quantified as 3.0 x 1.1 cm.
* The diagram highlights the use of both MR and CT imaging in the diagnostic process.
* The time frame for the "*maurosis fugax*" event is obscured, limiting the information available.
* The phrases following "Radiology:", "MR HEAD:", and "CT HEAD:" are incomplete, indicated by ellipses.
### Interpretation
The diagram illustrates a typical diagnostic pathway for a stroke. The patient presents with symptoms (right weakness and aphasia), undergoes consultation to gather medical history and assess symptoms, then proceeds to examination including radiological imaging (MR and CT scans). The initial suspicion of a stroke is refined through imaging, leading to a final diagnosis of hemorrhagic stroke. The hematoma size provides a quantifiable measure of the stroke's severity. The incomplete phrases suggest that further details regarding the imaging findings and the patient's condition are available but not fully presented in this diagram. The diagram emphasizes the importance of a systematic approach to stroke diagnosis, utilizing both clinical assessment and advanced imaging techniques.
</details>
Figure 1: When a patient is admitted, an initial consultation takes place to collect subjective information. Subsequent observations may then require further examination to confirm the diagnosis.
## 2 Related Works
Natural language explanation. Recent advancements in NLP have led to significant achievements [Min et al., 2023]. However, existing models often lack explainability, posing potential risks [Danilevsky et al., 2020, Gurrapu et al., 2023]. Numerous efforts have been made to address this challenge. One effective approach is to provide a human-understandable plain text explanation alongside the model’s output [Camburu et al., 2018, Rajani et al., 2019]. Another strategy involves identifying evidence within the input that serves as a rationale for the model’s decisions, aligning with human reasoning [DeYoung et al., 2020]. Expanding on this concept, [Jhamtani and Clark, 2020] introduces chain-structured explanations, given that a diagnosis can demand multi-hop reasoning. This idea is further refined by ProofWriter [Tafjord et al., 2021] through a proof stage for explanations, and by [Zhao et al., 2021] through retrieval from a corpus. [Dalvi et al., 2021] proposes the entailment tree, offering more detailed explanations and facilitating inspection of the model’s reasoning. More recently, [Zhang et al., 2024] employed cumulative reasoning to tap into the potential of LLMs to provide explanation via a directed acyclic graph. Although substantial progress has been made, interpreting NLP tasks in medical domains remains an ongoing challenge [Liévin et al., 2024].
Benchmarks of interpretability in the medical domain Several datasets are designed to assess a model’s reasoning together with its interpretability in medical NLP (Table 1). MedMCQA [Pal et al., 2022] and other medical QA datasets [Li et al., 2023, Chen et al., 2024] provide plain text as explanations for QA tasks. NLI4CT [Jullien et al., 2023] uses clinical trial reports, focusing on NLI supported by multi-hop reasoning. N2N2 [Gao et al., 2022] proposes a summarization (Sum) task for a diagnosis based on multiple pieces of evidence in the input clinical note. NEJM CPC [Zack et al., 2023] interprets clinicians’ diagnostic reasoning as plain text for reasoning clinical diagnosis (CD). DR.BENCH [Gao et al., 2023b] aggregates publicly available datasets to assess the diagnostic reasoning of LLMs. Utilizing an multi-evidence entailment tree explanation, DiReCT introduces a more rigorous task to assess whether LLMs can align with doctors’ reasoning in real clinical settings.
Table 1: Comparison of existing datasets for medical reasoning tasks and ours. “t” and “w” mean tokens and words for the length of input, respectively.
| Dataset | Task | Data Source | Length | Explanation | # Cases |
| --- | --- | --- | --- | --- | --- |
| MedMCQA [Pal et al., 2022] | QA | Examination | 9.93 t | Plain Text | 194,000 |
| ExplainCPE [Li et al., 2023] | QA | Examination | 37.79 w | Plain Text | 7,000 |
| JAMA Challenge [Chen et al., 2024] | QA | Clinical Cases | 371 w | Plain Text | 1,524 |
| Medbullets [Chen et al., 2024] | QA | Online Questions | 163 w | Plain Text | 308 |
| N2N2 [Gao et al., 2022] | Sum | Clinical Notes | 785.46 t | Evidences | 768 |
| NLI4CT [Jullien et al., 2023] | NLI | Clinical Trail Reports | 10-35 t | Multi-hop | 2,400 |
| NEJM CPC [Zack et al., 2023] | CD | Clinical Cases | - | Plain Text | 2,525 |
| DiReCT (Ours) | CD | Clinical Notes | 1074.6 t | Entailment Tree | 511 |
## 3 A benchmark for Clinical Notes Diagnosis
This section first detail clinical notes (Section 3.1). We also describes the knowledge graph that encodes existing guidelines (Section 3.2). Our task definition, which tasks a clinical note and the knowledge graph as input is given in Section 3.4. We then present our annotation process for clinical notes (Section 3.3) and the evaluation metrics (Section 3.5).
### 3.1 Clinical Notes
Clinical notes used in DiReCT are stored in the SOAP format [Weed, 1970]. A clinical note comprises four components: In the subjective section, the physician records the patient’s chief complaint, the history of present illness, and other subjective experiences reported by the patient. The objective section contains structural data obtained through examinations (inspection, auscultation, etc.) and other measurable means. The assessment section involves the physician’s analysis and evaluation of the patient’s condition. This may include a summary of current status, etc. Finally, the plan section outlines the physician’s proposed treatment and management plan. This may include prescribed medications, recommended therapies, and further investigations. A clinical note also includes a primary discharge diagnosis (PDD) in the assessment section.
DiReCT’s clinical notes are sourced from the MIMIC-IV dataset [Johnson et al., 2023] (PhysioNet Credentialed Health Data License 1.5.0), which encompasses over 40,000 patients admitted to the intensive care units. Each note contains clinical data for a patient. To construct DiReCT, we curated a subset of 511 notes whose PDDs fell within one of 25 disease categories $i$ in 5 medical domains.
In our task, a note $R=\{r\}$ is an excerpt of 6 clinical data in the subjective and objective sections (i.e., $|R|=6$ ): chief complaint, history of present illness, past medical history, family history, physical exam, and pertinent results. We excluded data, such as review system and social history, because they are often missing in the original clinical notes and are less relevant to the diagnosis. We also identified the PDD $d^⋆$ associated with $R$ . All clinical notes in DiReCT are related to only one PDD, and there is no secondary discharge diagnosis. The set of $d^⋆$ ’s for all $R$ ’s collectively forms $D^⋆$ . We manually removed any descriptions that disclose the PDD in $R$ .
### 3.2 Diagnostic Knowledge Graph
Existing knowledge graphs for the medical domain, e.g., UMLS KG [Bodenreider, 2004], lack the ability to provide specific clinical decision support (e.g., diagnostic threshold, context-specific data, dosage information, etc.), which are critical for accurate diagnosis.
Our knowledge graphs $K=\{K_i\}_i$ is a collection of graph $K_i$ for disease category $i$ . $K_i$ is based on the diagnosis criteria in existing guidelines (refer to supplementary material for details). $K_i$ ’s nodes are either premise $p∈P_i$ (medical statement, e.g., Headache is a symptom of) and diagnoses $d∈D_i$ (e.g., Suspected Stroke). $K_i$ consists of two different types of edges. One is premise-to-diagnosis edges $S_i=\{(p,d)\}$ , where $p∈P_i$ and $d∈D_i$ ; an edge is from $p$ to $d$ . This edge represents the necessary premise $p$ to make a diagnosis $d$ . We refer to them as supporting edges. The other is diagnosis-to-diagnosis edges $F_i=\{(d,d^\prime)\}$ , where $d,d^\prime∈D_i$ and the edge is from $d$ to $d^\prime$ , which represents the diagnostic flow. These edges are referred to as procedural edges.
A disease category is defined according to an existing guideline, which starts from a certain diagnosis; therefore, a procedural graph $G_i=(D_i,F_i)$ has only one root node and arbitrarily branches toward multiple leaf nodes that represent PDDs (i.e., the clinical notes in DiReCT are chosen to cover all leaf nodes of $G_i$ ). Thus, $G_i$ is a tree. We denote the set of the leaf nodes (or PDDs) as $D^⋆_i⊂D_i$ . The knowledge graph is denoted by $K_i=(D_i,P_i,S_i,F_ i)$ .
<details>
<summary>x2.png Details</summary>
### Visual Description
\n
## Diagram: Acute Coronary Syndrome (ACS) Diagnostic Pathway
### Overview
The image depicts a flowchart illustrating a diagnostic pathway for Acute Coronary Syndrome (ACS). It outlines the progression from initial symptoms and findings to different classifications of ACS, based on criteria like ST elevation, troponin levels, and ECG results. The diagram uses rectangular boxes to represent diagnostic categories or findings, and arrows to indicate the flow of assessment and diagnosis.
### Components/Axes
The diagram does not have traditional axes. It consists of interconnected boxes representing clinical states and findings. The flow is directional, indicated by arrows. The key components are:
* **Initial Presentations:** Breathlessness, Arrhythmias, Third Heart Sound, Any Severe Presentations
* **Intermediate Diagnoses:** Suspected ACS, Strongly Suspected ACS, non-ST Elevation
* **Final Diagnoses:** STEMI-ACS, NSTEMI-ACS, NSTE-ACS, UA (Unstable Angina)
* **Tests/Criteria:** ST Elevation, hs-cTn (high-sensitivity Troponin), Cardiac Troponin, No Obvious ECG
### Detailed Analysis or Content Details
The diagram can be broken down into sections:
**Left Side - Initial Assessment:**
* "Breathlessness is a symptom..." leads to "Suspected ACS".
* "Arrhythmias is..." leads to "Suspected ACS".
* "Third Heart Sound..." leads to "Suspected ACS".
* "Any Severe Presentations..." leads to "Strongly Suspected ACS".
**Central Pathway:**
* "Suspected ACS" leads to both "Strongly Suspected ACS" and "NSTE-ACS".
* "Strongly Suspected ACS" leads to "STEMI-ACS" (via a red arrow) and "NSTE-ACS" (via a red arrow).
* "non-ST Elevation..." leads to "NSTE-ACS".
**Right Side - Further Refinement:**
* "ST Elevation is criteria..." leads to "STEMI-ACS".
* "hs-cTn Exceeded..." leads to "NSTEMI-ACS".
* "Cardiac Troponin" leads to "NSTEMI-ACS".
* "NSTE-ACS" leads to "UA" (via a red arrow) and "NSTEMI-ACS" (via a blue arrow).
* "No Obvious ECG..." leads to "UA".
The arrows are color-coded: blue arrows indicate a more direct or positive association, while red arrows suggest a less direct or alternative pathway. The "..." notation suggests that the phrases are incomplete.
### Key Observations
* The diagram highlights the importance of ST elevation and troponin levels in differentiating between types of ACS.
* The pathway is not strictly linear; there are multiple routes to different diagnoses.
* The use of color-coded arrows suggests varying degrees of certainty or likelihood in the diagnostic process.
* The diagram focuses on a clinical decision-making process, rather than presenting quantitative data.
### Interpretation
This diagram represents a simplified clinical algorithm for the diagnosis of Acute Coronary Syndrome. It illustrates how clinicians progress through a series of assessments – initial symptoms, ECG findings, and biomarker levels – to arrive at a specific diagnosis. The branching pathways reflect the complexity of ACS and the need for careful evaluation to determine the appropriate treatment strategy.
The distinction between STEMI-ACS (ST-Elevation Myocardial Infarction) and NSTEMI-ACS (Non-ST-Elevation Myocardial Infarction) is crucial, as STEMI typically requires immediate reperfusion therapy. The diagram emphasizes that the presence of ST elevation is a key criterion for STEMI diagnosis.
The inclusion of "Unstable Angina" (UA) as a possible diagnosis indicates that not all patients with suspected ACS will have evidence of myocardial damage (elevated troponin levels).
The "..." notation suggests that the diagram is a simplified representation of a more complex clinical reality. In practice, clinicians consider a wide range of factors when diagnosing and managing ACS. The diagram serves as a useful tool for understanding the basic principles of ACS diagnosis, but it should not be used as a substitute for clinical judgment.
</details>
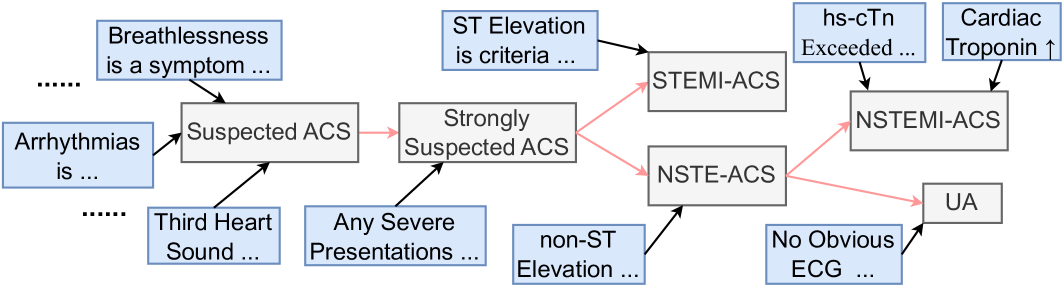
Figure 2: A part of $K_i$ for $i$ being Acute Coronary Syndromes.
Figure 2 shows a part of $K_i$ , where $i$ is Acute Coronary Syndromes (ACS). Premises in $P_i$ and diagnoses in $D_i$ are given in the blue and gray boxes, while PDDs in $D^⋆_i$ are ones without outgoing edges (i.e., STEMI-ACS and NSTEMI-ACS, and UA). The black and red arrows are edges in $S$ and $F$ , respectively, where the black arrows indicate the supporting edges.
$K$ serves two essential functions: (1) They serve as the gold standard for annotation, guiding doctors in the precise and uniform interpretation of clinical notes. (2) Our task also allows a model to use them to ensure the output from an LLM can be closely aligned with the reasoning processes of medical professionals.
### 3.3 Data Annotation
Let $d^⋆∈D^⋆_i$ denote the PDD of disease category $i$ associated with $R$ . We can find a subgraph $K_i(d^⋆)$ of $K_i$ that contains all ancestors of $d^⋆$ , including premises in $P_i$ . We also denote the set of supporting edges in $K_i(d^⋆)$ as $S_i(d^⋆)$ . Our annotation process is, for each supporting edge $(p,d)∈S_i(d^⋆)$ , to extract observation $o∈O$ in $R$ (highlighted text in the clinical note in Figure 3) and provide rationalization $z$ of this deduction why $o$ is a support for $d$ or corresponds to $p$ . All annotations strictly follow the procedural flow in $K_i$ , and each observation is only related to one diagnostic node. If $R$ does not provide sufficient observations for the PDD (which may happen when a certain test is omitted), the annotators were asked to add plausible observations to $R$ . This choice compromises the fidelity of our dataset to the original clinical notes, but we chose it for the completeness of the dataset. They form the explanation $E=\{(o,z,d)\}$ for $(R,d^⋆)$ . This annotation process was carried out by 9 clinical physicians and subsequently verified for accuracy and completeness by three senior medical experts.
Table 2: Statistics of DiReCT.
| Medical domain | # cat. | # samples | $|D_i|$ | $|D^⋆_i|$ | $|O|$ | Length |
| --- | --- | --- | --- | --- | --- | --- |
| Cardiology | 7 | 184 | 27 | 16 | 8.7 | 1156.6 t |
| Gastroenterology | 4 | 103 | 11 | 7 | 4.3 | 1026.0 t |
| Neurology | 5 | 77 | 17 | 11 | 11.9 | 1186.3 t |
| Pulmonology | 5 | 92 | 26 | 17 | 10.7 | 940.7 t |
| Endocrinology | 4 | 55 | 20 | 14 | 6.9 | 1063.5 t |
| Overall | 25 | 511 | 101 | 65 | 8.5 | 1074.6 t |
Table 2 summarizes statistics of our dataset. The second and third columns (“# cats.” and “# samples”) show the numbers of disease categories and samples in the respective medical domains. $|D_i|$ and $|D_i^⋆|$ are the total numbers of diagnoses (diseases) and PDDs, summed over all diagnostic categories in the medical domain, respectively. $|O|$ is the average number of annotated observations. “Length” is the average number of tokens in $R$ .
<details>
<summary>x3.png Details</summary>
### Visual Description
\n
## Diagram: Heart Failure Diagnostic Pathway
### Overview
This diagram illustrates a diagnostic pathway for heart failure (HF), linking clinical notes and findings to rationale and eventual diagnosis. The diagram uses a flow chart style with arrows indicating relationships between clinical observations, underlying reasons, and diagnostic outcomes. The left side presents a clinical note with redacted information, the center provides rationale for suspicion, and the right side shows the diagnostic outcomes.
### Components/Axes
The diagram is divided into three main sections:
1. **Clinical Note:** A block of text representing patient medical information.
2. **Rationale:** A list of statements linking clinical findings to potential diagnoses.
3. **Diagnosis:** A flowchart showing the progression from suspected HF to specific HF diagnoses.
The diagram includes connecting arrows, indicating the flow of information from clinical observations to rationale and then to diagnosis.
### Detailed Analysis or Content Details
**Clinical Note (Left Side):**
The clinical note contains redacted patient information. Visible keywords include:
* **Chief Complaint:** Scrotal and leg swelling
* **History of Present Illness:** Mentions swelling over 3 days, admission with acute CHF, EKG consistent with NSR, NANI, and left ventricle enlargement.
* **Past Medical History:** Diabetes, Hypertension, CKD stage 3, GERD, Depression, Amputation, Pneumonia, Osteoarthritis, History of Asthma.
* **Family History:** No family history of artery disease.
* **Physical Exam:** Lung findings (bibasilar rales), abdominal findings, pitting edema, HEENT, AT/NC, EOMI, PERRL.
* **Pertinent Results:** 03:50PM BLOOD WBC-8.0 RBC-3.26 Hgb-9.3 Hct-30.9 MCHC-29.9, 11:30AM Blood proBNP-3843, Overall left ventricular systolic function is mildly depressed (LVEF= 45-50%), imaging suggests increased filling pressure (PCWP=***Hg).
**Rationale (Center):**
* Peripheral edema is a sign of heart failure.
* Hypertension is the risk factor for heart failure.
* NT-proBNP 3843±125pg/ml is a diagnostic criteria of strong HF.
* Cardiac structure abnormalities are diagnostic criteria of heart failure.
* Cardiac systolic dysfunction <49% can lead to the diagnosis of HFmEF.
**Diagnosis (Right Side):**
* **Suspected HF** (Top box) - connected to Peripheral edema and Hypertension.
* **Strongly Suspected HF** (Middle box) - connected to NT-proBNP and Cardiac structure abnormalities.
* **HF** (Central box) - connected to Strongly Suspected HF.
* **HFmEF** (Bottom box) - connected to HF and Cardiac systolic dysfunction.
### Key Observations
* The diagram highlights a clear pathway from clinical presentation (edema, hypertension) to biochemical markers (NT-proBNP) and imaging findings (LVEF, PCWP) leading to a diagnosis of heart failure.
* The use of "±" in the NT-proBNP value suggests a range or uncertainty in the measurement.
* The diagram suggests that a combination of clinical findings and diagnostic tests is necessary to arrive at a diagnosis.
* The diagram focuses on HFmEF (Heart Failure with mildly reduced Ejection Fraction) as a potential outcome.
### Interpretation
This diagram represents a simplified clinical decision-making process for heart failure. It demonstrates how a physician might integrate information from a patient's history, physical exam, and laboratory/imaging results to arrive at a diagnosis. The diagram emphasizes the importance of considering multiple factors, rather than relying on a single test or finding. The flow from clinical note to rationale to diagnosis suggests a Bayesian approach to diagnosis, where initial observations inform probabilities that are updated with further evidence. The diagram's focus on HFmEF reflects the increasing recognition of this subtype of heart failure, which often presents with subtle symptoms and can be challenging to diagnose. The redacted information in the clinical note suggests that this diagram is intended as a general illustration of the diagnostic process, rather than a specific case study.
</details>
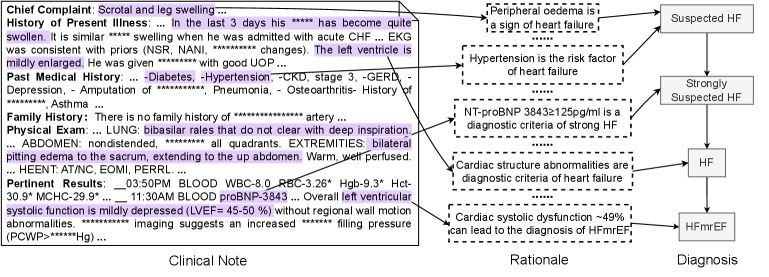
Figure 3: An annotation sample of Heart Failure (HF). The left part is the clinical note alongside extracted observations by a doctor. The middle part outlines the steps of the rationale for the premise corresponding to each diagnostic node shown in the right part.
### 3.4 Task Definition
We propose two tasks with different levels of supplied external knowledge. The first task is, given $R$ and $G$ , to predict the associated PDD $d^⋆$ and generate an explanation $E$ that explains the model’s diagnostic procedure from $R$ to $d^⋆$ , i.e., letting $M$ denote a model:
$$
\displaystyle\hat{d}^⋆,\hat{E}=M(R,G), \tag{1}
$$
where $\hat{d}^⋆∈∪_iD^⋆_i$ and $\hat{E}$ are predictions for the PDD and explanation, respectively. With this task, the knowledge of specific diagnostic procedures in existing guidelines can be used for prediction, facilitating interpretability. The second task takes $K$ as input instead of $G$ , i.e.,:
$$
\displaystyle\hat{d}^⋆,\hat{E}=M(R,K). \tag{2}
$$
This task allows for the use of broader knowledge of premises for prediction. One may also try a task without any external knowledge.
### 3.5 Evaluation Metrics
We designed three metrics to quantify the predictive performance over our benchmark.
(1) Accuracy of diagnosis $\textit{Acc}^diag$ evaluates if a model can correctly identify the diagnosis. $\textit{Acc}^diag=1$ if $d^⋆=\hat{d}$ , and $\textit{Acc}^diag=0$ otherwise. The average is reported.
(2) Completeness of observations $\textit{Obs}^comp$ evaluates whether a model extracts all and only necessary observations for the prediction. Let $O$ and $\hat{O}$ denote the sets of observations in $E$ and $\hat{E}$ , respectively. The metric is defined as $\textit{Obs}^comp=|O∩\hat{O}|/|O∪ \hat{O}|$ , where the numerator is the number of observations that are common in both $O$ and $\hat{O}$ . We find the common observations with an LLM (refer to the supplementary material for more detail). This metric simultaneously evaluates the correctness of each observation and the coverage. To supplement it, we also report the precision $\textit{Obs}^pre$ and recall $\textit{Obs}^rec$ , given by $\textit{Obs}^pre=|O∩\hat{O}|/|\hat{O}|$ and $\textit{Obs}^rec=|O∩\hat{O}|/|O|$ .
(3) Faithfulness of explanations Faith evaluates if the diagnostic flow toward the PDD is fully supported by observations with faithful rationalizations. This involves establishing a one-to-one correspondence between deductions in the prediction and the ground truth. We use the correspondences established for computing $\textit{Obs}^comp$ . Let $o∈O$ and $\hat{o}∈\hat{O}$ denote corresponding observations. This correspondence is considered successful if $z$ and $\hat{z}$ as well as $d$ and $\hat{d}$ associated with $o$ and $\hat{o}$ matches. Let $m(E,\hat{E})$ denote the number of successful matches. We use the ratio of $m(E,\hat{E})$ to $|O∩\hat{O}|$ and $|O∪\hat{O}|$ as evaluation metrics $\textit{Exp}^com$ and $\textit{Exp}^all$ , respectively, to see failures come from observations or explanations and diagnosis.
## 4 Baseline
<details>
<summary>x4.png Details</summary>
### Visual Description
\n
## Diagram: Clinical Note Reasoning Process
### Overview
This diagram illustrates a process for reasoning from a clinical note to a diagnosis, utilizing observations and a diagnostic knowledge graph (KG). The process involves perception, narrowing down information, rationale generation, and iterative reasoning steps.
### Components/Axes
The diagram consists of the following components:
* **Clinical Note:** Represented by a document icon with plus and minus symbols, and a list of components:
* r₁: Chief Complaint
* r₂: History of Present Illness
* r₃: Past Medical History
* r₄: Family History
* r₅: Physical Examination
* r₆: Pertinent Results
* **Perception & Narrowing-down:** A process block connecting the Clinical Note to Observations.
* **Observations:** A numbered list of clinical findings:
* ① Elevated blood pressures
* ② CXR showed mild pulmonary edema
* ③ CHF/Cardiomyopathy
* ④ Severe LV diastolic dysfunction
* ⑤ BPs: 148/98, 156/93
* ...... (indicating more observations exist)
* **Rationale:** A block labeled "Rationale" connected to the Observations and the Reasoning blocks.
* **Reasoning:** Three stacked blocks labeled "Reasoning", connected by a looping arrow, indicating iterative processing.
* **Diagnostic KG:** A graph consisting of nodes labeled a1 through a5, connected by edges.
* **Connections:** Arrows indicating the flow of information between components. Dashed arrows connect Observations to Reasoning blocks.
### Detailed Analysis or Content Details
The diagram depicts a flow of information starting from a Clinical Note. The note is processed through "Perception" and "Narrowing-down" to generate "Observations". These observations (①-⑤) are then used to generate a "Rationale". The rationale, along with the observations, feeds into a "Reasoning" block. The reasoning process is iterative, as indicated by the looping arrow connecting the three Reasoning blocks. The Diagnostic KG appears to provide background knowledge used in the reasoning process.
Specifically:
* **Observation ⑤** provides specific blood pressure readings: 148/98 and 156/93.
* The Diagnostic KG contains 5 nodes: a1, a2, a3, a4, and a5.
* Each Reasoning block receives input from the Observations (①-⑤) and the Rationale.
* The output of each Reasoning block is fed back into the next iteration of the Reasoning process.
### Key Observations
* The process is iterative, suggesting that the reasoning process refines the diagnosis over multiple steps.
* The Diagnostic KG plays a central role in the reasoning process, providing contextual knowledge.
* The diagram does not specify the nature of the "Rationale" or the specific reasoning mechanisms employed.
* The "......" after Observation ⑤ indicates that the list of observations is not exhaustive.
### Interpretation
This diagram illustrates a simplified model of clinical reasoning. It suggests that a clinician begins with a comprehensive clinical note, extracts relevant observations, and then uses these observations, along with background knowledge (represented by the Diagnostic KG), to generate a rationale and arrive at a diagnosis. The iterative nature of the reasoning process highlights the importance of considering multiple factors and refining the diagnosis based on new information. The diagram emphasizes the transition from raw clinical data to a reasoned conclusion. The use of a knowledge graph suggests a move towards more structured and formalized approaches to clinical decision-making. The diagram is conceptual and does not provide details on the specific algorithms or methods used for perception, narrowing-down, rationale generation, or reasoning.
</details>
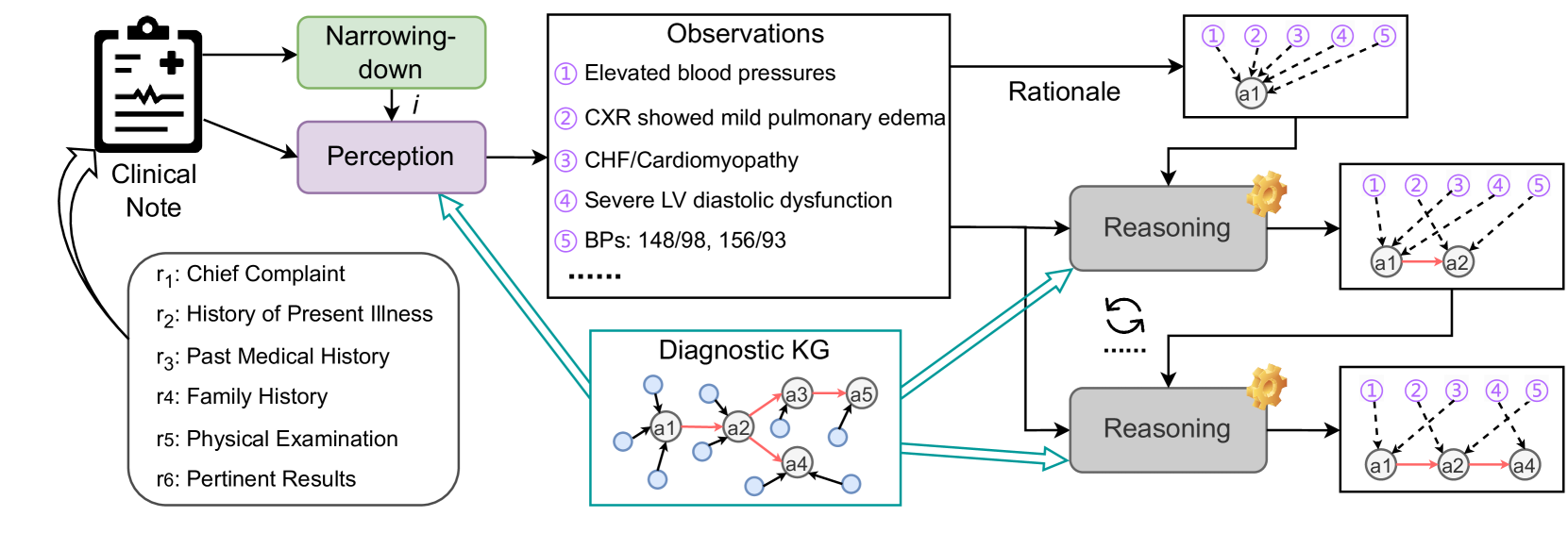
Figure 4: Pipeline of our baseline. The dotted line in the right-most boxes means deductions from an observation to a diagnosis.
Figure 4 shows an overview of our baseline with three LLM-based modules narrowing-down, perception, and reasoning (refer to the supplementary material for more details). The narrowing-down module $U$ takes $R$ as input to make a prediction $\hat{i}$ of the disease category, i.e., $\hat{i}=U(R)$ .
Let $d_t∈D_\hat{i}$ be the diagnosis that has been reached with $t$ iterations over $K_\hat{i}$ , where $t$ corresponds to the depth of node $d_t$ and so is less than or equal to the depth of $K_i$ . $d_0$ is the root node of $K_\hat{i}$ . For $d_0$ , we apply the perception module to extract all observations in $R$ and explanation $E_0$ to support $d_0$ as
$$
\displaystyle\hat{O},\hat{E_0}=W(d_0,K_\hat
{i}). \tag{3}
$$
$K_\hat{i}$ is supplied to facilitate the model to extract all observations for the following reasoning process. We used only pairs of an observation and a premise. We abuse $K$ to mean this for notation simplicity.
Diagnosis $d_t$ identifies the set $\{d_n\}_n$ of its children and so the set $P_\hat{i}(\{d_n\}_n)=\{p∈P_i|(p,d_n)∈ S_i,d_n∈\{d_n\}\}$ of premises that support $d_n$ . Therefore, our reasoning module $V$ iteratively and greedily identifies the next step’s diagnosis (i.e., $d_t+1$ ) from $\{d_n\}_n$ , making a rationalization for each deduction. That is, $V$ verifies whether there exist $o$ ’s in $\hat{O}$ that supports one $d_n$ . If $d_n$ is fully supported, $d_n$ is identified as $d_t+1$ for the $(t+1)$ -th iteration, i.e.,
$$
\displaystyle d_t+1,\hat{E}_t+1=V(\hat{O},\{d_n\},
P_\hat{i}(\{d_n\}_n)). \tag{4}
$$
Otherwise, the reasoning module fails. $V$ is repeated until $d_t^\prime$ in $D^⋆_\hat{i}$ is found or it fails. In our annotation, each observation contributes to deducing only one $d_t$ . Therefore, if an observation in $\hat{E}_t+1$ is included in the preceding sets of explanations $\hat{E}_0$ to $\hat{E}_t$ , the corresponding explanation in the preceding sets is removed.
## 5 Experiments
### 5.1 Experimental Setup
We assess the reasoning capabilities of 7 recent LLMs from diverse families and model sizes, including 5 instruction-tuned models that are openly accessible: LLama3 8B and 70B [AI@Meta, 2024], Zephyr 7B [Tunstall et al., 2023], Mistral 7B [Jiang et al., 2023], and Mixtral 8 $×$ 7B [Jiang et al., 2023]. We have also obtained access to private versions of the GPT-3.5 turbo [OpenAI, 2023b] and GPT-4 turbo [OpenAI, 2023a] These two models are housed on a HIPPA-compliant instance within Microsoft Azure AI Studio. No data is transferred to either Microsoft or OpenAI. This secure environment enables us to safely conduct experiments with the MIMIC-IV dataset, in compliance with the Data Use Agreement., which are high-performance closed-source models. Each LLM is utilized to implement our baseline’s narrowing-down, perception, and reasoning modules. The temperature is set to 0. For computing evaluation metrics, we use LLama3 8B with few-shot prompts to make correspondences between $O$ and $\hat{O}$ as well as to verify a match between predicted and ground-truth explanations (refer to the supplementary material for more details).
### 5.2 Results
Comparison among LLMs. Table 3 shows the performance of our baseline built on top of various LLMs. We first evaluate a variant of our task that takes graph $G=\{G_i\}$ consisting of only procedural flow as external knowledge instead of $K$ . Comparison between $G$ and $K$ demonstrates the importance of supplying premises with the model and LLMs’ capability to make use of extensive external knowledge that may be superficially different from statements in $R$ . Subsequently, some models are evaluated with our task using $K$ . In addition to the metrics in Section 3.5, we also adopt the accuracy of disease category $\textit{Acc}^cat$ , which gives 1 when $\hat{i}=i$ , as our baseline’s performance depends on it.
Table 3: Diagnostic reasoning ability of different LLMs under the proposed baseline method.
| | | Diagnosis | Observation | Explanation | | | | |
| --- | --- | --- | --- | --- | --- | --- | --- | --- |
| Task | Models | Acc ${}^cat$ | Acc ${}^diag$ | $\textit{Obs}^pre$ | $\textit{Obs}^rec$ | $\textit{Obs}^comp$ | $\textit{Exp}^com$ | $\textit{Exp}^all$ |
| With $G$ | Zephyr 7B | 0.274 | 0.151 | 0.123 ${}_±0.200$ | 0.115 ${}_±0.166$ | 0.092 ${}_±0.108$ | 0.071 ${}_±0.139$ | 0.014 ${}_±0.037$ |
| Mistral 7B | 0.507 | 0.306 | 0.211 ${}_±0.190$ | 0.317 ${}_±0.253$ | 0.173 ${}_±0.157$ | 0.230 ${}_±0.312$ | 0.062 ${}_±0.088$ | |
| Mixtral 8 $×$ 7B | 0.413 | 0.237 | 0.147 ${}_±0.165$ | 0.266 ${}_±0.261$ | 0.124 ${}_±0.138$ | 0.144 ${}_±0.268$ | 0.029 ${}_±0.056$ | |
| LLama3 8B | 0.576 | 0.321 | 0.253 ${}_±0.156$ | 0.437 ${}_±0.207$ | 0.219 ${}_±0.137$ | 0.232 ${}_±0.316$ | 0.071 ${}_±0.093$ | |
| LLama3 70B | 0.752 | 0.540 | 0.277 ${}_±0.146$ | 0.537 ${}_±0.192$ | 0.256 ${}_±0.142$ | 0.395 ${}_±0.320$ | 0.112 ${}_±0.110$ | |
| GPT-3.5 turbo | 0.679 | 0.455 | 0.389 ${}_±0.212$ | 0.351 ${}_±0.192$ | 0.275 ${}_±0.167$ | 0.331 ${}_±0.366$ | 0.103 ${}_±0.127$ | |
| GPT-4 turbo | 0.772 | 0.572 | 0.446 ${}_±0.207$ | 0.491 ${}_±0.180$ | 0.371 ${}_±0.186$ | 0.475 ${}_±0.363$ | 0.199 ${}_±0.181$ | |
| With $K$ | LLama3 8B | 0.576 | 0.344 | 0.235 ${}_±0.162$ | 0.394 ${}_±0.227$ | 0.199 ${}_±0.142$ | 0.327 ${}_±0.375$ | 0.087 ${}_±0.114$ |
| LLama3 70B | 0.735 | 0.581 | 0.262 ${}_±0.146$ | 0.501 ${}_±0.208$ | 0.236 ${}_±0.131$ | 0.463 ${}_±0.374$ | 0.125 ${}_±0.117$ | |
| GPT-3.5 turbo | 0.652 | 0.413 | 0.347 ${}_±0.241$ | 0.279 ${}_±0.203$ | 0.232 ${}_±0.184$ | 0.374 ${}_±0.408$ | 0.121 ${}_±0.152$ | |
| GPT-4 turbo | 0.781 | 0.614 | 0.431 ${}_±0.207$ | 0.458 ${}_±0.187$ | 0.353 ${}_±0.170$ | 0.633 ${}_±0.338$ | 0.247 ${}_±0.201$ | |
Table 4: Evaluation of diagnostic reasoning ability of LLMs when no external knowledge is provided.
| | | | Observation | Explanation | | | |
| --- | --- | --- | --- | --- | --- | --- | --- |
| Task | Models | Acc ${}^diag$ | $\textit{Obs}^pre$ | $\textit{Obs}^rec$ | $\textit{Obs}^comp$ | $\textit{Exp}^com$ | $\textit{Exp}^all$ |
| With $D^⋆$ | LLama3 8B | 0.070 | 0.154 ${}_±0.139$ | 0.330 ${}_±0.244$ | 0.135 ${}_±0.122$ | 0.020 ${}_±0.100$ | 0.004 ${}_±0.016$ |
| LLama3 70B | 0.502 | 0.257 ${}_±0.150$ | 0.509 ${}_±0.213$ | 0.237 ${}_±0.145$ | 0.138 ${}_±0.209$ | 0.034 ${}_±0.054$ | |
| GPT-3.5 turbo | 0.223 | 0.164 ${}_±0.242$ | 0.149 ${}_±0.212$ | 0.116 ${}_±0.174$ | 0.091 ${}_±0.231$ | 0.025 ${}_±0.065$ | |
| GPT-4 turbo | 0.636 | 0.461 ${}_±0.206$ | 0.482 ${}_±0.160$ | 0.378 ${}_±0.174$ | 0.186 ${}_±0.221$ | 0.074 ${}_±0.090$ | |
| No Knowledge | LLama3 8B | 0.023 | 0.137 ${}_±0.159$ | 0.258 ${}_±0.274$ | 0.119 ${}_±0.141$ | 0.018 ${}_±0.083$ | 0.006 ${}_±0.026$ |
| LLama3 70B | 0.037 | 0.246 ${}_±0.148$ | 0.504 ${}_±0.222$ | 0.227 ${}_±0.148$ | 0.022 ${}_±0.093$ | 0.007 ${}_±0.030$ | |
| GPT-3.5 turbo | 0.059 | 0.161 ${}_±0.238$ | 0.148 ${}_±0.215$ | 0.113 ${}_±0.171$ | 0.036 ${}_±0.131$ | 0.011 ${}_±0.039$ | |
| GPT-4 turbo | 0.074 | 0.410 ${}_±0.208$ | 0.443 ${}_±0.191$ | 0.324 ${}_±0.182$ | 0.047 ${}_±0.143$ | 0.019 ${}_±0.058$ | |
With $G$ , we can see that GPT-4 achieves the best performance in most metrics, especially related to observations and explanations, surpassing LLama3 70B by a large margin. In terms of accuracy (in both category and diagnosis levels), LLama3 70B is comparable to GPT-4. LLama3 70B also has a higher $\textit{Obs}^rec$ but low $\textit{Obs}^pre$ and $\textit{Obs}^comp$ , which means that this model tends to extract many observations. Models with high diagnostic accuracy are not necessarily excel in finding essential information in long text (i.e., observations) and generating reasons (i.e., explanations).
When $K$ is given, all models show better diagnostic accuracy (except GPT-3.5) and explanations, while observations are slightly degraded. GPT-4 with $K$ enhances Acc ${}^diag$ , $\textit{Exp}^com$ , and $\textit{Exp}^all$ scores. This suggests that premises and supporting edges are beneficial for diagnosis and explanation. Lower observational performance may indicate that the models lack the ability to associate premises and text in $R$ , which are often superficially different though semantically consistent.
LLMs may undergo inherent challenges for evaluation when no external knowledge is supplied. They may have the knowledge to diagnose but cannot make consistent observations and explanations that our task expects through $K$ . To explore this, we evaluate two settings: (1) giving $D^⋆$ and (2) no knowledge is supplied to a model (shown in Table 4). The prompts used for this setup are detailed in the supplementary material. We do not evaluate the accuracy of disease category prediction as it is basically the same as Table 3. We can clearly see that with $D^⋆$ , GPT-4’s diagnostic and observational scores are comparable to those of the task with $K$ , though explanatory performance is much worse. Without any external knowledge, the diagnostic accuracy is also inferior. We understand this comparison is unfair, as the prompts differ. We intend to give a rough idea about the challenge without external knowledge. The deteriorated performance can be attributed to inconsistent wording of diagnosis names, which makes evaluation tough. High observational scores imply that observations in $R$ can be identified without relying on external knowledge. There can be some cues to spot them.
<details>
<summary>x5.png Details</summary>
### Visual Description
## Bar Chart: Performance Comparison of LLMs Across Medical Specialties
### Overview
The image presents a series of five bar charts, each representing the performance of three Large Language Models (LLMs) – LLama3, GPT-3.5, and GPT-4 – across five different medical specialties: Cardiology, Gastroenterology, Neurology, Pulmonology, and Endocrinology. The performance is measured by three metrics: Accuracy (Acc), Completeness (Comp), and Faithfulness (Faith). Each bar chart displays the values of these metrics for each LLM within a specific specialty.
### Components/Axes
* **X-axis:** Represents the LLM models: LLama3, GPT-3.5, and GPT-4.
* **Y-axis:** Represents the performance scores, ranging from 0.0 to 1.0.
* **Legend (Top-Center):**
* Green: Acc (Accuracy)
* Yellow: Comp (Completeness)
* Light Blue: Faith (Faithfulness)
* **Chart Titles (Bottom):** Each chart is labeled with the corresponding medical specialty.
### Detailed Analysis
**1. Cardiology**
* LLama3: Acc ≈ 0.32, Comp ≈ 0.16, Faith ≈ 0.08
* GPT-3.5: Acc ≈ 0.44, Comp ≈ 0.24, Faith ≈ 0.16
* GPT-4: Acc ≈ 0.48, Comp ≈ 0.32, Faith ≈ 0.24
**2. Gastroenterology**
* LLama3: Acc ≈ 0.28, Comp ≈ 0.12, Faith ≈ 0.04
* GPT-3.5: Acc ≈ 0.56, Comp ≈ 0.28, Faith ≈ 0.16
* GPT-4: Acc ≈ 0.72, Comp ≈ 0.44, Faith ≈ 0.28
**3. Neurology**
* LLama3: Acc ≈ 0.24, Comp ≈ 0.16, Faith ≈ 0.12
* GPT-3.5: Acc ≈ 0.76, Comp ≈ 0.52, Faith ≈ 0.32
* GPT-4: Acc ≈ 0.84, Comp ≈ 0.60, Faith ≈ 0.40
**4. Pulmonology**
* LLama3: Acc ≈ 0.28, Comp ≈ 0.16, Faith ≈ 0.08
* GPT-3.5: Acc ≈ 0.48, Comp ≈ 0.28, Faith ≈ 0.16
* GPT-4: Acc ≈ 0.56, Comp ≈ 0.36, Faith ≈ 0.24
**5. Endocrinology**
* LLama3: Acc ≈ 0.20, Comp ≈ 0.12, Faith ≈ 0.04
* GPT-3.5: Acc ≈ 0.36, Comp ≈ 0.20, Faith ≈ 0.12
* GPT-4: Acc ≈ 0.44, Comp ≈ 0.28, Faith ≈ 0.16
### Key Observations
* GPT-4 consistently outperforms both LLama3 and GPT-3.5 across all medical specialties and all metrics.
* LLama3 generally exhibits the lowest performance across all categories.
* Accuracy (Acc) scores are generally higher than Completeness (Comp) and Faithfulness (Faith) scores for all models and specialties.
* The largest performance differences between models are observed in Neurology and Gastroenterology.
* Faithfulness scores are consistently the lowest across all specialties and models.
### Interpretation
The data suggests that GPT-4 is the most capable LLM for medical applications, demonstrating superior accuracy, completeness, and faithfulness compared to GPT-3.5 and LLama3. The consistent outperformance of GPT-4 highlights the importance of model size and training data quality in achieving reliable performance in specialized domains like medicine. The lower faithfulness scores across all models suggest a potential area for improvement, indicating that these models may sometimes generate responses that are not entirely grounded in factual information. The variability in performance across different medical specialties suggests that the complexity and available data within each specialty may influence the LLM's ability to perform effectively. The relatively low performance of LLama3 indicates that it may not be suitable for complex medical tasks without further refinement. The gap between accuracy and faithfulness suggests that while the models can often provide correct answers, they may not always be able to justify or support those answers with reliable evidence.
</details>
Figure 5: Performance of LLama3 70B, GPT-3.5, and GPT-4 under different medical domains. We use the task with $G$ .
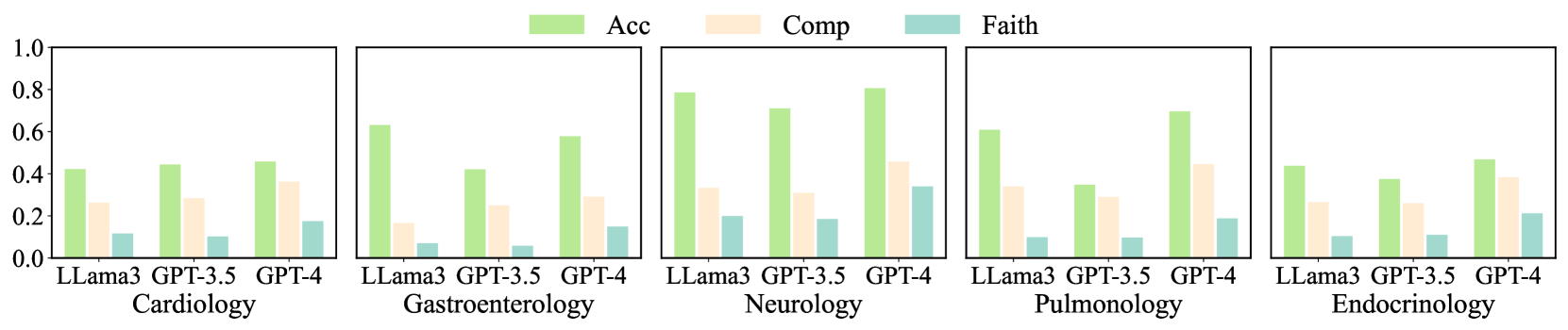
Performance in individual domains. Figure 5 summarizes the performance of LLama3 70B, GPT-3.5, and GPT-4 across different medical domains, evaluated using Acc ${}^cat$ , $\textit{Obs}^comp$ , and $\textit{Exp}^all$ . Neurology gives the best diagnostic accuracy, where GPT-4 achieved an accuracy of 0.806. LLama3 also performed well (0.786). In terms of $\textit{Obs}^comp$ and $\textit{Exp}^all$ , GPT-4’s results were 0.458 and 0.340, respectively, with the smallest difference between the two scores among all domains. This smaller gap indicates that in Neurology, the common observations in prediction and ground truth lead to the correct diagnoses with faithful rationalizations. However, GPT-4 yields a higher diagnostic accuracy score while a lower explanatory score, suggesting that the observations captured by the model or their rationalizations differ from human doctors.
For Cardiology and Endocrinology, the diagnostic accuracy of the models is relatively low (GPT-4 achieved 0.458 and 0.468, respectively). Nevertheless, $\textit{Obs}^comp$ and $\textit{Exp}^all$ are relatively high. Endocrinology results in lower diagnostic accuracy and higher explanatory performance. A smaller gap may imply that in these two domains, successful predictions are associated with observations similar to those of human doctors, and the reasoning process may be analogous. Conversely, in Gastroenterology, higher Acc ${}^cat$ ) is accompanied by lower $\textit{Obs}^comp$ and $\textit{Exp}^all$ (especially for LLama3), potentially indicating a significant divergence in the reasoning process from human doctors. Overall, DiReCT demonstrates that the degree of alignment between the model’s diagnostic reasoning ability and that of human doctors varies across different medical domains.
Table 5: Consistency of automated evaluation metrics with human judgments.
| Model | Observation | Rationalization |
| --- | --- | --- |
| LLama3 8B | 0.887 | 0.801 |
| GPT-4 turbo | 0.902 | 0.836 |
Reliability of automatic evaluation. We randomly pick out 100 samples from DiReCT and their prediction by GPT-4 over the task with $G$ to assess the consistency of our automated metrics to evaluate the observational and explanatory performance in Section 3.3 to human judgments. Three physicians joined this experiment. For each prediction $\hat{o}∈\hat{O}$ , they are asked to find a similar observation in ground truth $O$ . For explanatory metrics, they verify if each prediction $\hat{z}∈\hat{E}$ for $\hat{o}∈\hat{O}$ align with ground-truth $z∈E$ corresponding to $o$ . A prediction and a ground truth are deemed aligned for both assessments if at least two specialists agree. We compare LLama3’s and GPT-4’s judgments to explore if there is a gap between these LLMs. As summarized in Table 5, GPT-4 achieves the best results, with LLama3 8B also displaying a similar performance. From these results, we argue that our automated evaluation metrics are consistent with human judgments, and LLama3 is sufficient for this evaluation, allowing the cost-efficient option.
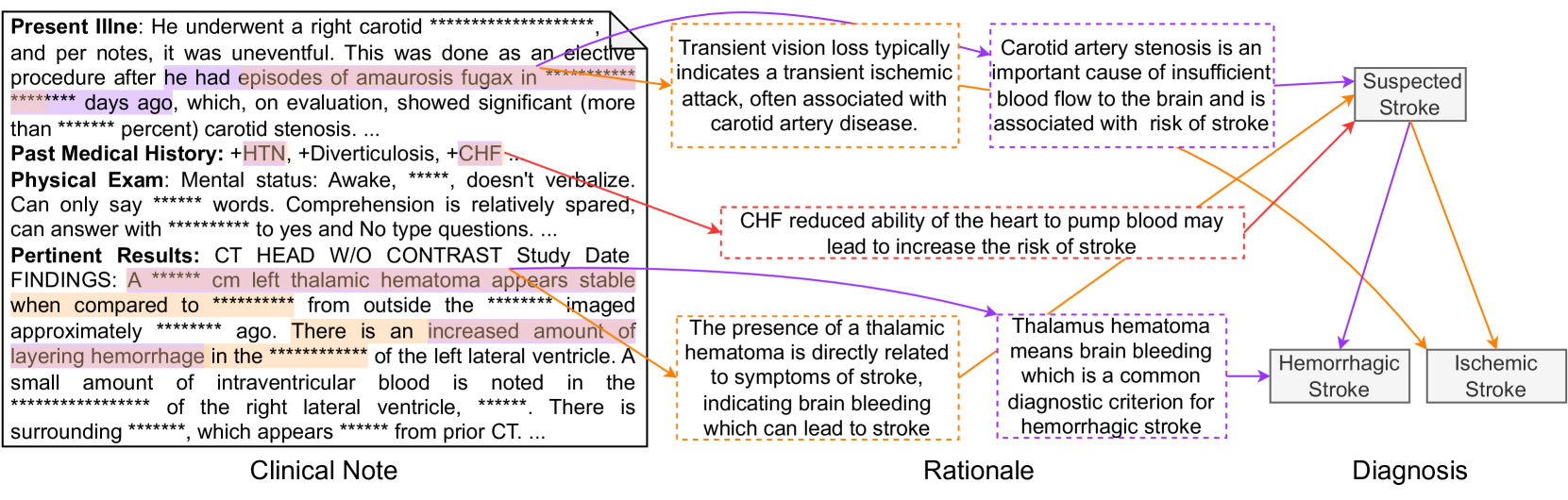
A prediction example. Figure 6 shows a sample generated by GPT-4. The ground-truth PDD of the input clinical note is Hemorrhagic Stroke. In this figure, purple, orange, and red indicate explanations only in the ground truth, only in prediction, and common in both, respectively; therefore, red is a successful prediction of an explanation, while purple and orange are a false negative and false positive. GPT-4 treats the observation of aurosis fugax as the criteria for diagnosing Ischemic Stroke. However, this observation only supports Suspected Stroke. Conversely, observation thalamic hematoma, which is the key indicator of Hemorrhagic Stroke, is regarded as a less important clue. Such observation-diagnosis correspondence errors lead to the model’s misdiagnosis. More samples are available in the supplementary material.
<details>
<summary>x6.png Details</summary>
### Visual Description
\n
## Diagram: Clinical Reasoning for Stroke Diagnosis
### Overview
This diagram illustrates the clinical reasoning process for diagnosing stroke, linking clinical notes, rationale, and potential diagnoses (suspected stroke, hemorrhagic stroke, ischemic stroke). It presents a flow of information from patient presentation (Clinical Note) through the underlying medical reasoning (Rationale) to the final diagnostic possibilities (Diagnosis). The diagram uses colored arrows to indicate the relationships between these elements.
### Components/Axes
The diagram is divided into three main sections, positioned horizontally:
* **Clinical Note** (Left): Contains patient medical information.
* **Rationale** (Center): Explains the medical reasoning connecting the clinical note to the diagnosis.
* **Diagnosis** (Right): Lists potential diagnoses.
The diagram uses arrows to show the flow of information. Red arrows indicate a connection to "Suspected Stroke" and "Hemorrhagic Stroke", while purple arrows indicate a connection to "Ischemic Stroke".
### Detailed Analysis or Content Details
**Clinical Note:**
The clinical note contains the following information, with some values obscured by asterisks:
* **Present Illness:** Patient underwent a right carotid procedure, was uneventful. Episodes of amaurosis fugax for approximately `******` days, which showed significant (more than `******` percent) carotid stenosis.
* **Past Medical History:** +HTN, +Diverticulosis, +CHF.
* **Physical Exam:** Mental status: Awake, `******`, doesn't verbalize. Can only say `******` words. Comprehension is relatively spared, can answer with `******` to yes and no type questions.
* **Pertinent Results: CT HEAD W/O CONTRAST Study Date FINDINGS:** A `******` cm left thalamic hematoma appears stable when compared to `******` from outside the `******` imaged approximately `******` ago. There is an increased amount of layering hemorrhage in the `******` of the left lateral ventricle. A small amount of intraventricular blood is noted in the `******` of the right lateral ventricle, `******`. There is surrounding `******`, which appears from prior CT.
**Rationale:**
* Transient vision loss typically indicates a transient ischemic attack, often associated with carotid artery disease.
* Carotid artery stenosis is an important cause of insufficient blood flow to the brain and is associated with risk of stroke.
* CHF reduced ability of the heart to pump blood may lead to increase the risk of stroke.
* The presence of a thalamic hematoma is directly related to symptoms of stroke, indicating brain bleeding which can lead to stroke.
* Thalamus hematoma means brain bleeding which is a common diagnostic criterion for hemorrhagic stroke.
**Diagnosis:**
* Suspected Stroke
* Hemorrhagic Stroke
* Ischemic Stroke
**Arrow Connections:**
* The Clinical Note connects to "Suspected Stroke" via a red arrow.
* The Clinical Note connects to "Hemorrhagic Stroke" via a red arrow.
* The Rationale section connects to "Hemorrhagic Stroke" via a red arrow.
* The Rationale section connects to "Ischemic Stroke" via a purple arrow.
### Key Observations
The diagram highlights the connection between carotid stenosis, CHF, and thalamic hematoma to the potential diagnoses of stroke. The presence of a thalamic hematoma strongly suggests hemorrhagic stroke. The diagram emphasizes the importance of considering both ischemic and hemorrhagic stroke in the differential diagnosis.
### Interpretation
This diagram represents a simplified model of clinical reasoning in stroke diagnosis. It demonstrates how a physician integrates patient history, physical exam findings, and imaging results to arrive at a diagnosis. The diagram emphasizes the importance of considering multiple potential diagnoses and the need to weigh the evidence carefully. The obscured values (`******`) indicate that this is likely a template or example, and specific patient data would fill in those gaps. The use of color-coded arrows helps to visually represent the strength of the association between different elements. The diagram suggests that the patient's presentation (Clinical Note) points towards both ischemic and hemorrhagic stroke possibilities, requiring further investigation to differentiate between the two. The rationale section provides the medical basis for these diagnostic considerations. The diagram is a useful tool for illustrating the diagnostic process and for educating healthcare professionals.
</details>
Figure 6: An example prediction for a clinical note with PDD of Hemorrhagic Stroke by GPT-4.
## 6 Conclusion and Limitations
We proposed DiReCT as the first benchmark for evaluating the diagnostic reasoning ability of LLMs with interpretability by supplying external knowledge as a graph. Our evaluations reveal a notable disparity between current leading-edge LLMs and human experts, underscoring the urgent need for AI models that can perform reliable and interpretable reasoning in clinical environments. DiReCT can be easily extended to more challenging settings by removing the knowledge graph from the input, facilitating evaluations of future LLMs.
Limitations. DiReCT encompasses only a subset of disease categories and considers only one PDD, omitting the inter-diagnostic relationships due to their complexity—a significant challenge even for human doctors. Additionally, our baseline may not use optimal prompts, chain-of-thought reasoning, or address issues related to hallucinations in task responses. Our dataset is solely intended for model evaluation but not for use in clinical environments. The use of the diagnostic knowledge graph is also limited to serving merely as a part of input. Future work will focus on constructing a more comprehensive disease dataset and developing an extensive diagnostic knowledge graph.
## Acknowledgments and Disclosure of Funding
This work was supported by World Premier International Research Center Initiative (WPI), MEXT, Japan. This work is also supported by JSPS KAKENHI 24K20795 and Dalian Haichuang Project for Advanced Talents.
## References
- Zhao et al. [2023] Wayne Xin Zhao, Kun Zhou, Junyi Li, Tianyi Tang, Xiaolei Wang, Yupeng Hou, Yingqian Min, Beichen Zhang, Junjie Zhang, Zican Dong, Yifan Du, Chen Yang, Yushuo Chen, Zhipeng Chen, Jinhao Jiang, Ruiyang Ren, Yifan Li, Xinyu Tang, Zikang Liu, Peiyu Liu, Jian-Yun Nie, and Ji-Rong Wen. A survey of large language models. arXiv preprint arXiv:2303.18223, 2023.
- Min et al. [2023] Bonan Min, Hayley Ross, Elior Sulem, Amir Pouran Ben Veyseh, Thien Huu Nguyen, Oscar Sainz, Eneko Agirre, Ilana Heintz, and Dan Roth. Recent advances in natural language processing via large pre-trained language models: A survey. ACM Computing Surveys, 56(2):1–40, 2023.
- Anil et al. [2023] Rohan Anil, Andrew M Dai, Orhan Firat, Melvin Johnson, Dmitry Lepikhin, Alexandre Passos, Siamak Shakeri, Emanuel Taropa, Paige Bailey, Zhifeng Chen, et al. Palm 2 technical report. arXiv preprint arXiv:2305.10403, 2023.
- Han et al. [2023] Tianyu Han, Lisa C Adams, Jens-Michalis Papaioannou, Paul Grundmann, Tom Oberhauser, Alexander Löser, Daniel Truhn, and Keno K Bressem. Medalpaca–an open-source collection of medical conversational ai models and training data. arXiv preprint arXiv:2304.08247, 2023.
- Jin et al. [2021] Di Jin, Eileen Pan, Nassim Oufattole, Wei-Hung Weng, Hanyi Fang, and Peter Szolovits. What disease does this patient have? a large-scale open domain question answering dataset from medical exams. Applied Sciences, 11(14):6421, 2021.
- OpenAI [2023a] OpenAI. GPT-4 Technical Report. CoRR, abs/2303.08774, 2023a. doi: 10.48550/arXiv.2303.08774. URL https://doi.org/10.48550/arXiv.2303.08774.
- Bubeck et al. [2023] Sébastien Bubeck, Varun Chandrasekaran, Ronen Eldan, Johannes Gehrke, Eric Horvitz, Ece Kamar, Peter Lee, Yin Tat Lee, Yuanzhi Li, Scott Lundberg, et al. Sparks of artificial general intelligence: Early experiments with gpt-4. arXiv preprint arXiv:2303.12712, 2023.
- Nori et al. [2023] Harsha Nori, Nicholas King, Scott Mayer McKinney, Dean Carignan, and Eric Horvitz. Capabilities of gpt-4 on medical challenge problems. arXiv preprint arXiv:2303.13375, 2023.
- Liévin et al. [2024] Valentin Liévin, Christoffer Egeberg Hother, Andreas Geert Motzfeldt, and Ole Winther. Can large language models reason about medical questions? Patterns, 5(3), 2024.
- Pal et al. [2022] Ankit Pal, Logesh Kumar Umapathi, and Malaikannan Sankarasubbu. MedMCQA: A large-scale multi-subject multi-choice dataset for medical domain question answering. In Conference on health, inference, and learning, pages 248–260. PMLR, 2022.
- Li et al. [2023] Dongfang Li, Jindi Yu, Baotian Hu, Zhenran Xu, and Min Zhang. ExplainCPE: A free-text explanation benchmark of chinese pharmacist examination. arXiv preprint arXiv:2305.12945, 2023.
- Chen et al. [2024] Hanjie Chen, Zhouxiang Fang, Yash Singla, and Mark Dredze. Benchmarking large language models on answering and explaining challenging medical questions. arXiv preprint arXiv:2402.18060, 2024.
- Jullien et al. [2023] Mael Jullien, Marco Valentino, Hannah Frost, Paul O’Regan, Donal Landers, and André Freitas. Semeval-2023 task 7: Multi-evidence natural language inference for clinical trial data. arXiv preprint arXiv:2305.02993, 2023.
- Gao et al. [2023a] Yanjun Gao, Ruizhe Li, John Caskey, Dmitriy Dligach, Timothy Miller, Matthew M Churpek, and Majid Afshar. Leveraging a medical knowledge graph into large language models for diagnosis prediction. arXiv preprint arXiv:2308.14321, 2023a.
- Johnson et al. [2023] Alistair E. W. Johnson, Lucas Bulgarelli, Lu Shen, Alvin Gayles, Ayad Shammout, Steven Horng, Tom J. Pollard, Sicheng Hao, Benjamin Moody, Brian Gow, Li-wei H. Lehman, Leo A. Celi, and Roger G. Mark. MIMIC-IV, a freely accessible electronic health record dataset. Scientific data, 10(1):1, 2023.
- Xi et al. [2023] Zhiheng Xi, Wenxiang Chen, Xin Guo, Wei He, Yiwen Ding, Boyang Hong, Ming Zhang, Junzhe Wang, Senjie Jin, Enyu Zhou, Rui Zheng, Xiaoran Fan, Xiao Wang, Limao Xiong, Yuhao Zhou, Weiran Wang, Changhao Jiang, Yicheng Zou, Xiangyang Liu, Zhangyue Yin, Shihan Dou, Rongxiang Weng, Wensen Cheng, Qi Zhang, Wenjuan Qin, Yongyan Zheng, Xipeng Qiu, Xuanjing Huang, and Tao Gui. The rise and potential of large language model based agents: A survey, 2023.
- Tang et al. [2023] Xiangru Tang, Anni Zou, Zhuosheng Zhang, Yilun Zhao, Xingyao Zhang, Arman Cohan, and Mark Gerstein. Medagents: Large language models as collaborators for zero-shot medical reasoning. arXiv preprint arXiv:2311.10537, 2023.
- Middleton et al. [2013] Blackford Middleton, Meryl Bloomrosen, Mark A Dente, Bill Hashmat, Ross Koppel, J Marc Overhage, Thomas H Payne, S Trent Rosenbloom, Charlotte Weaver, and Jiajie Zhang. Enhancing patient safety and quality of care by improving the usability of electronic health record systems: recommendations from amia. Journal of the American Medical Informatics Association, 20(e1):e2–e8, 2013.
- Liu et al. [2022] Jinghui Liu, Daniel Capurro, Anthony Nguyen, and Karin Verspoor. “note bloat” impacts deep learning-based nlp models for clinical prediction tasks. Journal of biomedical informatics, 133:104149, 2022.
- Danilevsky et al. [2020] Marina Danilevsky, Kun Qian, Ranit Aharonov, Yannis Katsis, Ban Kawas, and Prithviraj Sen. A survey of the state of explainable AI for natural language processing. In Proceedings of the 1st Conference of the Asia-Pacific Chapter of the Association for Computational Linguistics and the 10th International Joint Conference on Natural Language Processing, pages 447–459, 2020.
- Gurrapu et al. [2023] Sai Gurrapu, Ajay Kulkarni, Lifu Huang, Ismini Lourentzou, and Feras A Batarseh. Rationalization for explainable nlp: A survey. Frontiers in Artificial Intelligence, 6, 2023.
- Camburu et al. [2018] Oana-Maria Camburu, Tim Rocktäschel, Thomas Lukasiewicz, and Phil Blunsom. e-snli: Natural language inference with natural language explanations. Advances in Neural Information Processing Systems, 31, 2018.
- Rajani et al. [2019] Nazneen Fatema Rajani, Bryan McCann, Caiming Xiong, and Richard Socher. Explain yourself! leveraging language models for commonsense reasoning. In Proceedings of the 57th Annual Meeting of the Association for Computational Linguistics, pages 4932–4942, Florence, Italy, 2019.
- DeYoung et al. [2020] Jay DeYoung, Sarthak Jain, Nazneen Fatema Rajani, Eric Lehman, Caiming Xiong, Richard Socher, and Byron C. Wallace. ERASER: A benchmark to evaluate rationalized NLP models. In Proceedings of the 58th Annual Meeting of the Association for Computational Linguistics, pages 4443–4458, 2020.
- Jhamtani and Clark [2020] Harsh Jhamtani and Peter Clark. Learning to explain: Datasets and models for identifying valid reasoning chains in multihop question-answering. In Proceedings of the 2020 Conference on Empirical Methods in Natural Language Processing, page 137–150, 2020.
- Tafjord et al. [2021] Oyvind Tafjord, Bhavana Dalvi Mishra, and Peter Clark. Proofwriter: Generating implications, proofs, and abductive statements over natural language. In Findings of the Association for Computational Linguistics: ACL-IJCNLP, page 3621–3634, 2021.
- Zhao et al. [2021] Chen Zhao, Chenyan Xiong, Jordan Boyd-Graber, and Hal Daumé III. Multi-step reasoning over unstructured text with beam dense retrieval. In Proceedings of the 2021 Conference of the North American Chapter of the Association for Computational Linguistics: Human Language Technologies, pages 4635–4641, 2021.
- Dalvi et al. [2021] Bhavana Dalvi, Peter Jansen, Oyvind Tafjord, Zhengnan Xie, Hannah Smith, Leighanna Pipatanangkura, and Peter Clark. Explaining answers with entailment trees. In Proceedings of the 2021 Conference on Empirical Methods in Natural Language Processing, pages 7358–7370, 2021.
- Zhang et al. [2024] Yifan Zhang, Jingqin Yang, Yang Yuan, and Andrew Chi-Chih Yao. Cumulative reasoning with large language models. In ICLR 2024 Workshop on Bridging the Gap Between Practice and Theory in Deep Learning, 2024. URL https://openreview.net/forum?id=XAAYyRxTlQ.
- Gao et al. [2022] Yanjun Gao, Dmitriy Dligach, Timothy Miller, Samuel Tesch, Ryan Laffin, Matthew M. Churpek, and Majid Afshar. Hierarchical annotation for building a suite of clinical natural language processing tasks: Progress note understanding. In Proceedings of the Thirteenth Language Resources and Evaluation Conference, pages 5484–5493, Marseille, France, 2022. European Language Resources Association.
- Zack et al. [2023] Travis Zack, Gurpreet Dhaliwal, Rabih Geha, Mary Margaretten, Sara Murray, and Julian C Hong. A clinical reasoning-encoded case library developed through natural language processing. Journal of General Internal Medicine, 38(1):5–11, 2023.
- Gao et al. [2023b] Yanjun Gao, Dmitriy Dligach, Timothy Miller, John Caskey, Brihat Sharma, Matthew M Churpek, and Majid Afshar. Dr. bench: Diagnostic reasoning benchmark for clinical natural language processing. Journal of Biomedical Informatics, 138:104286, 2023b.
- Weed [1970] L.L. Weed. Medical Records, Medical Education, and Patient Care: The Problem-oriented Record as a Basic Tool. Press of Case Western Reserve University, 1970. ISBN 9780815191889.
- Bodenreider [2004] Olivier Bodenreider. The unified medical language system (umls): integrating biomedical terminology. Nucleic acids research, 32(suppl_1):D267–D270, 2004.
- AI@Meta [2024] AI@Meta. Llama 3 model card. 2024. URL https://github.com/meta-llama/llama3/blob/main/MODEL_CARD.md.
- Tunstall et al. [2023] Lewis Tunstall, Edward Beeching, Nathan Lambert, Nazneen Rajani, Kashif Rasul, Younes Belkada, Shengyi Huang, Leandro von Werra, Clémentine Fourrier, Nathan Habib, et al. Zephyr: Direct distillation of lm alignment. arXiv preprint arXiv:2310.16944, 2023.
- Jiang et al. [2023] Albert Q Jiang, Alexandre Sablayrolles, Arthur Mensch, Chris Bamford, Devendra Singh Chaplot, Diego de las Casas, Florian Bressand, Gianna Lengyel, Guillaume Lample, Lucile Saulnier, et al. Mistral 7b. arXiv preprint arXiv:2310.06825, 2023.
- OpenAI [2023b] OpenAI. Introducing ChatGPT and Whisper APIs. 2023b. URL https://openai.com/blog/introducing-chatgpt-and-whisper-apis.
- Byrne et al. [2024] Robert A Byrne, Xavier Rossello, JJ Coughlan, Emanuele Barbato, Colin Berry, Alaide Chieffo, Marc J Claeys, Gheorghe-Andrei Dan, Marc R Dweck, Mary Galbraith, et al. 2023 esc guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the european society of cardiology (esc). European Heart Journal: Acute Cardiovascular Care, 13(1):55–161, 2024.
- Members et al. [2022] Writing Committee Members, Eric M Isselbacher, Ourania Preventza, James Hamilton Black III, John G Augoustides, Adam W Beck, Michael A Bolen, Alan C Braverman, Bruce E Bray, Maya M Brown-Zimmerman, et al. 2022 acc/aha guideline for the diagnosis and management of aortic disease: a report of the american heart association/american college of cardiology joint committee on clinical practice guidelines. Journal of the American College of Cardiology, 80(24):e223–e393, 2022.
- Joglar et al. [2024] José A Joglar, Mina K Chung, Anastasia L Armbruster, Emelia J Benjamin, Janice Y Chyou, Edmond M Cronin, Anita Deswal, Lee L Eckhardt, Zachary D Goldberger, Rakesh Gopinathannair, et al. 2023 acc/aha/accp/hrs guideline for the diagnosis and management of atrial fibrillation: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation, 149(1):e1–e156, 2024.
- Ommen et al. [2020] Steve R Ommen, Seema Mital, Michael A Burke, Sharlene M Day, Anita Deswal, Perry Elliott, Lauren L Evanovich, Judy Hung, José A Joglar, Paul Kantor, et al. 2020 aha/acc guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: executive summary: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Journal of the American College of Cardiology, 76(25):3022–3055, 2020.
- Heidenreich et al. [2022] Paul A Heidenreich, Biykem Bozkurt, David Aguilar, Larry A Allen, Joni J Byun, Monica M Colvin, Anita Deswal, Mark H Drazner, Shannon M Dunlay, Linda R Evers, et al. 2022 aha/acc/hfsa guideline for the management of heart failure: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Journal of the American College of Cardiology, 79(17):e263–e421, 2022.
- Su et al. [2021] Lilly Su, Rea Mittal, Devyani Ramgobin, Rahul Jain, and Rohit Jain. Current management guidelines on hyperlipidemia: the silent killer. Journal of lipids, 2021(1):9883352, 2021.
- Unger et al. [2020] Thomas Unger, Claudio Borghi, Fadi Charchar, Nadia A Khan, Neil R Poulter, Dorairaj Prabhakaran, Agustin Ramirez, Markus Schlaich, George S Stergiou, Maciej Tomaszewski, et al. 2020 international society of hypertension global hypertension practice guidelines. Hypertension, 75(6):1334–1357, 2020.
- Shah et al. [2021] Shailja C Shah, M Blanca Piazuelo, Ernst J Kuipers, and Dan Li. Aga clinical practice update on the diagnosis and management of atrophic gastritis: expert review. Gastroenterology, 161(4):1325–1332, 2021.
- Gyawali et al. [2024] C Prakash Gyawali, Rena Yadlapati, Ronnie Fass, David Katzka, John Pandolfino, Edoardo Savarino, Daniel Sifrim, Stuart Spechler, Frank Zerbib, Mark R Fox, et al. Updates to the modern diagnosis of gerd: Lyon consensus 2.0. Gut, 73(2):361–371, 2024.
- Kavitt et al. [2019] Robert T Kavitt, Anna M Lipowska, Adjoa Anyane-Yeboa, and Ian M Gralnek. Diagnosis and treatment of peptic ulcer disease. The American journal of medicine, 132(4):447–456, 2019.
- Barkun et al. [2019] Alan N Barkun, Majid Almadi, Ernst J Kuipers, Loren Laine, Joseph Sung, Frances Tse, Grigorios I Leontiadis, Neena S Abraham, Xavier Calvet, Francis KL Chan, et al. Management of nonvariceal upper gastrointestinal bleeding: guideline recommendations from the international consensus group. Annals of internal medicine, 171(11):805–822, 2019.
- McKhann et al. [1984] Guy McKhann, David Drachman, Marshall Folstein, Robert Katzman, Donald Price, and Emanuel M Stadlan. Clinical diagnosis of alzheimer’s disease: Report of the nincds-adrda work group* under the auspices of department of health and human services task force on alzheimer’s disease. Neurology, 34(7):939–939, 1984.
- Igaku-Shoin-Ltd. [2018] Igaku-Shoin-Ltd. Clinical practice guidelines for epilepsy 2018. 2018.
- Lipton et al. [2001] Richard B Lipton, Seymour Diamond, Michael Reed, Merle L Diamond, and Walter F Stewart. Migraine diagnosis and treatment: results from the american migraine study ii. Headache: The Journal of Head and Face Pain, 41(7):638–645, 2001.
- Lublin [2005] Fred D Lublin. Clinical features and diagnosis of multiple sclerosis. Neurologic clinics, 23(1):1–15, 2005.
- Kleindorfer et al. [2021] Dawn O Kleindorfer, Amytis Towfighi, Seemant Chaturvedi, Kevin M Cockroft, Jose Gutierrez, Debbie Lombardi-Hill, Hooman Kamel, Walter N Kernan, Steven J Kittner, Enrique C Leira, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the american heart association/american stroke association. Stroke, 52(7):e364–e467, 2021.
- Qaseem et al. [2011] Amir Qaseem, Timothy J Wilt, Steven E Weinberger, Nicola A Hanania, Gerard Criner, Thys van der Molen, Darcy D Marciniuk, Tom Denberg, Holger Schünemann, Wisia Wedzicha, et al. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the american college of physicians, american college of chest physicians, american thoracic society, and european respiratory society. Annals of internal medicine, 155(3):179–191, 2011.
- Gupta et al. [2013] Dheeraj Gupta, Ritesh Agarwal, Ashutosh Nath Aggarwal, VN Maturu, Sahajal Dhooria, KT Prasad, Inderpaul S Sehgal, Lakshmikant B Yenge, Aditya Jindal, Navneet Singh, et al. Guidelines for diagnosis and management of chronic obstructive pulmonary disease: Joint ics/nccp (i) recommendations. Lung India, 30(3):228–267, 2013.
- Olson and Davis [2020] Gregory Olson and Andrew M Davis. Diagnosis and treatment of adults with community-acquired pneumonia. Jama, 323(9):885–886, 2020.
- Konstantinides et al. [2020] Stavros V Konstantinides, Guy Meyer, Cecilia Becattini, Héctor Bueno, Geert-Jan Geersing, Veli-Pekka Harjola, Menno V Huisman, Marc Humbert, Catriona Sian Jennings, David Jiménez, et al. 2019 esc guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the european respiratory society (ers) the task force for the diagnosis and management of acute pulmonary embolism of the european society of cardiology (esc). European heart journal, 41(4):543–603, 2020.
- Lewinsohn et al. [2017] David M Lewinsohn, Michael K Leonard, Philip A LoBue, David L Cohn, Charles L Daley, Ed Desmond, Joseph Keane, Deborah A Lewinsohn, Ann M Loeffler, Gerald H Mazurek, et al. Official american thoracic society/infectious diseases society of america/centers for disease control and prevention clinical practice guidelines: diagnosis of tuberculosis in adults and children. Clinical Infectious Diseases, 64(2):e1–e33, 2017.
- Charmandari et al. [2014] Evangelia Charmandari, Nicolas C Nicolaides, and George P Chrousos. Adrenal insufficiency. The Lancet, 383(9935):2152–2167, 2014.
- ElSayed et al. [2023] Nuha A ElSayed, Grazia Aleppo, Vanita R Aroda, Raveendhara R Bannuru, Florence M Brown, Dennis Bruemmer, Billy S Collins, Kenneth Cusi, Marisa E Hilliard, Diana Isaacs, et al. 4. comprehensive medical evaluation and assessment of comorbidities: Standards of care in diabetes—2023. Diabetes Care, 46(Suppl 1):s49, 2023.
- Tritos and Miller [2023] Nicholas A Tritos and Karen K Miller. Diagnosis and management of pituitary adenomas: a review. Jama, 329(16):1386–1398, 2023.
- AlexanderErik et al. [2017] K AlexanderErik, N PearceElizabeth, A BrentGregory, S BrownRosalind, A GrobmanWilliam, H LazarusJohn, J MandelSusan, P PeetersRobin, et al. 2017 guidelines of the american thyroid association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid, 2017.
## Appendix A Details of DiReCT
### A.1 Data Statistics
Table 6: Disease statistics of DiReCT.
| Domains | Categories | # samples | $|D_i|$ | $|D^⋆_i|$ | References |
| --- | --- | --- | --- | --- | --- |
| Cardiology | Acute Coronary Syndromes | 65 | 6 | 3 | [Byrne et al., 2024] |
| Aortic Dissection | 14 | 3 | 2 | [Members et al., 2022] | |
| Atrial Fibrillation | 10 | 3 | 2 | [Joglar et al., 2024] | |
| Cardiomyopathy | 9 | 5 | 4 | [Ommen et al., 2020] | |
| Heart Failure | 52 | 6 | 3 | [Heidenreich et al., 2022] | |
| Hyperlipidemia | 2 | 2 | 1 | [Su et al., 2021] | |
| Hypertension | 32 | 2 | 1 | [Unger et al., 2020] | |
| Gastroenterology | Gastritis | 27 | 5 | 3 | [Shah et al., 2021] |
| Gastroesophageal Reflux Disease | 41 | 2 | 1 | [Gyawali et al., 2024] | |
| Peptic Ulcer Disease | 28 | 3 | 2 | [Kavitt et al., 2019] | |
| Upper Gastrointestinal Bleeding | 7 | 2 | 1 | [Barkun et al., 2019] | |
| Neurology | Alzheimer | 10 | 2 | 1 | [McKhann et al., 1984] |
| Epilepsy | 8 | 3 | 2 | [Igaku-Shoin-Ltd., 2018] | |
| Migraine | 4 | 3 | 2 | [Lipton et al., 2001] | |
| Multiple Sclerosis | 27 | 6 | 4 | [Lublin, 2005] | |
| Stroke | 28 | 3 | 2 | [Kleindorfer et al., 2021] | |
| Pulmonology | Asthma | 13 | 7 | 5 | [Qaseem et al., 2011] |
| COPD | 19 | 6 | 4 | [Gupta et al., 2013] | |
| Pneumonia | 20 | 4 | 2 | [Olson and Davis, 2020] | |
| Pulmonary Embolism | 35 | 5 | 3 | [Konstantinides et al., 2020] | |
| Tuberculosis | 5 | 3 | 2 | [Lewinsohn et al., 2017] | |
| Endocrinology | Adrenal Insufficiency | 20 | 4 | 3 | [Charmandari et al., 2014] |
| Diabetes | 13 | 4 | 2 | [ElSayed et al., 2023] | |
| Pituitary | 12 | 4 | 3 | [Tritos and Miller, 2023] | |
| Thyroid Disease | 10 | 6 | 4 | [AlexanderErik et al., 2017] | |
Table 6 provides a detailed breakdown of the disease categories included in DiReCT. The column labeled # samples indicates the number of data points. The symbols $|D_i|$ and $|D^⋆_i|$ denote the total number of diagnoses (diseases) and PDDs, respectively. Existing guidelines for diagnosing diseases were used as References, forming the foundation for constructing the diagnostic knowledge graphs. As some premise may not included in the referred guidelines. During annotation, physicians will incorporate their own knowledge to complete the knowledge graph.
### A.2 Structure of Knowledge Graph
The entire knowledge graph, denoted as $K$ , is stored in separate JSON files, each corresponding to a specific disease category $i$ as $K_i$ . Each $K_i$ comprises a procedural graph $G_i$ and the corresponding premise $p$ for each disease. As illustrated in Figure 7, the procedural graph $G_i$ is stored under the key "Diagnostic" in a dictionary structure. A key with an empty list as its value indicates a leaf diagnostic node as $d^⋆$ . The premise for each disease is saved under the key of "Knowledge" with the corresponding disease name as an index. For all the root nodes (e.g., Suspected Heart Failure), we further divide the premise into "Risk Factors", "Symptoms", and "Signs". Note that each premise is separated by ";".
<details>
<summary>x7.png Details</summary>
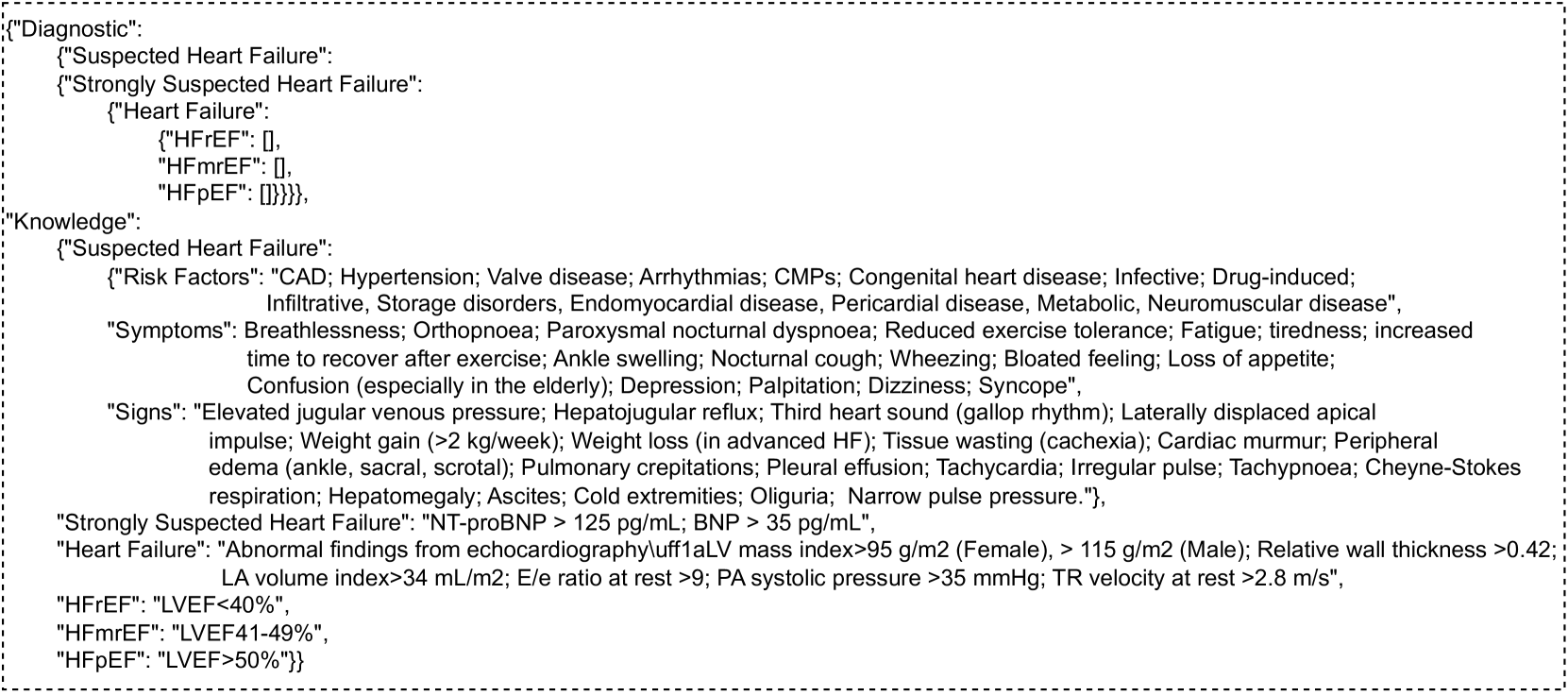
### Visual Description
## JSON Data: Heart Failure Diagnostic and Knowledge Base
### Overview
The image presents a JSON (JavaScript Object Notation) data structure containing information related to heart failure diagnosis and associated knowledge. The data is organized into nested objects representing "Diagnostic" criteria and "Knowledge" about heart failure.
### Components/Axes
The structure consists of key-value pairs. The keys are strings representing categories (e.g., "Diagnostic", "Knowledge", "Suspected Heart Failure", "Symptoms", "Signs"). The values are either strings, numbers, or nested JSON objects/arrays. There are no axes or scales in the traditional sense, as this is a data structure, not a chart or graph.
### Detailed Analysis or Content Details
**1. "Diagnostic" Section:**
* **"Suspected Heart Failure"**: Empty object `{}`.
* **"Strongly Suspected Heart Failure"**: Empty object `{}`.
* **"Heart Failure"**: Contains three sub-keys:
* **"HFrEF"**: Value is `0`. (Heart Failure with reduced Ejection Fraction)
* **"HFmrEF"**: Value is `0`. (Heart Failure with mildly reduced Ejection Fraction)
* **"HFpEF"**: Empty object `{}`. (Heart Failure with preserved Ejection Fraction)
**2. "Knowledge" Section:**
* **"Suspected Heart Failure"**:
* **"Risk Factors"**: A string listing: `"CAD; Hypertension; Valve disease; Arrhythmias; CMPs; Congenital heart disease; Infective; Drug-induced; Infiltrative; Storage disorders, Endomyocardial disease, Pericardial disease, Metabolic, Neuromuscular disease"`.
* **"Symptoms"**: A string listing: `"Breathlessness; Orthopnoea; Paroxysmal nocturnal dyspnoea; Reduced exercise tolerance; Fatigue; Tiredness; Increased time to recover after exercise; Ankle swelling; Nocturnal cough; Wheezing; Bloated feeling; Loss of appetite; Confusion (especially in the elderly); Depression; Palpitation; Dizziness; Syncope"`.
* **"Signs"**: A string listing: `"Elevated jugular venous pressure; Hepatjugular reflux; Third heart sound (gallop rhythm); Laterally displaced apical impulse; Weight gain (≥ 2 kg/week); Weight loss (in advanced HF); Tissue wasting (cachexia); Cardiac murmur; Peripheral edema (ankle, sacral, scrotal); Pulmonary crepitations; Pleural effusion; Tachycardia; Irregular pulse; Tachypnoea; Cheyne-Stokes respiration; Hepatomegaly; Ascites; Cold extremities; Oliguria; Narrow pulse pressure."`.
* **"Strongly Suspected Heart Failure"**:
* **"NT-proBNP"**: `"NT-proBNP > 125 pg/ml; BNP > 35 pg/ml"`.
* **"Heart Failure"**:
* **"Abnormal findings from echocardiography/uff1aLV mass index>95 g/m2 (Female), > 115 g/m2 (Male); Relative wall thickness >0.42; LA volume index>34 mL/m2; E/e ratio at rest >9; PA systolic pressure >35 mmHg; TR velocity at rest >2.8 m/s"**.
* **"HFrEF"**: `"LVEF<40%"`. (Left Ventricular Ejection Fraction)
* **"HFmrEF"**: `"LVEF41-49%"`.
* **"HFpEF"**: `"LVEF>50%"`.
### Key Observations
* The "Diagnostic" section indicates that, based on this data, there is no definitive diagnosis of any specific type of heart failure (HFrEF, HFmrEF, HFpEF) as the values are either 0 or empty objects.
* The "Knowledge" section provides a comprehensive list of risk factors, symptoms, and signs associated with heart failure.
* Specific biomarker thresholds (NT-proBNP, BNP) are provided for "Strongly Suspected Heart Failure".
* Echocardiographic criteria are listed for "Heart Failure".
* Ejection fraction ranges are defined for each heart failure subtype (HFrEF, HFmrEF, HFpEF).
### Interpretation
This JSON data represents a structured knowledge base and diagnostic framework for heart failure. It outlines the criteria used to suspect and diagnose heart failure, categorizing it into different subtypes based on ejection fraction. The data suggests a tiered approach to diagnosis, starting with identifying risk factors and symptoms, progressing to biomarker assessment, and culminating in echocardiographic evaluation. The empty values in the "Diagnostic" section suggest that this data represents a preliminary assessment or a case where further investigation is needed to reach a definitive diagnosis. The detailed lists of symptoms, signs, and risk factors are valuable for clinical decision-making and patient education. The inclusion of specific numerical thresholds (e.g., NT-proBNP levels, ejection fraction ranges) provides objective criteria for diagnosis and classification.
</details>
Figure 7: A sample of knowledge graph for Heart Failure. Each premise under the key of "Knowledge" is separated with ";".
### A.3 Annotation and Tools
We have developed proprietary software for annotation purposes. As depicted in Figure 8, annotators are presented with the original text as observations $o$ and are required to provide rationales ( $z$ ) to explain why a particular observation $o$ supports a disease $d$ . The left section of the figure, labeled Input1 to Input6, corresponds to different parts of the clinical note, specifically the chief complaint, history of present illness, past medical history, family history, physical exam, and pertinent results, respectively. Annotators will add the raw text into the first layer by left-clicking and dragging to select the original text, then right-clicking to add it. After each observation, a white box will be used to record the rationales. Finally, a connection will be made from each rationale to a disease, represented in a grey box. The annotation process strictly follow the knowledge graph. Both the final annotation and the raw clinical note will be saved in a JSON file. We provide the code to compile these annotations and detailed instructions for using our tool on GitHub.
<details>
<summary>extracted/5772958/Images_spp/annotation.png Details</summary>
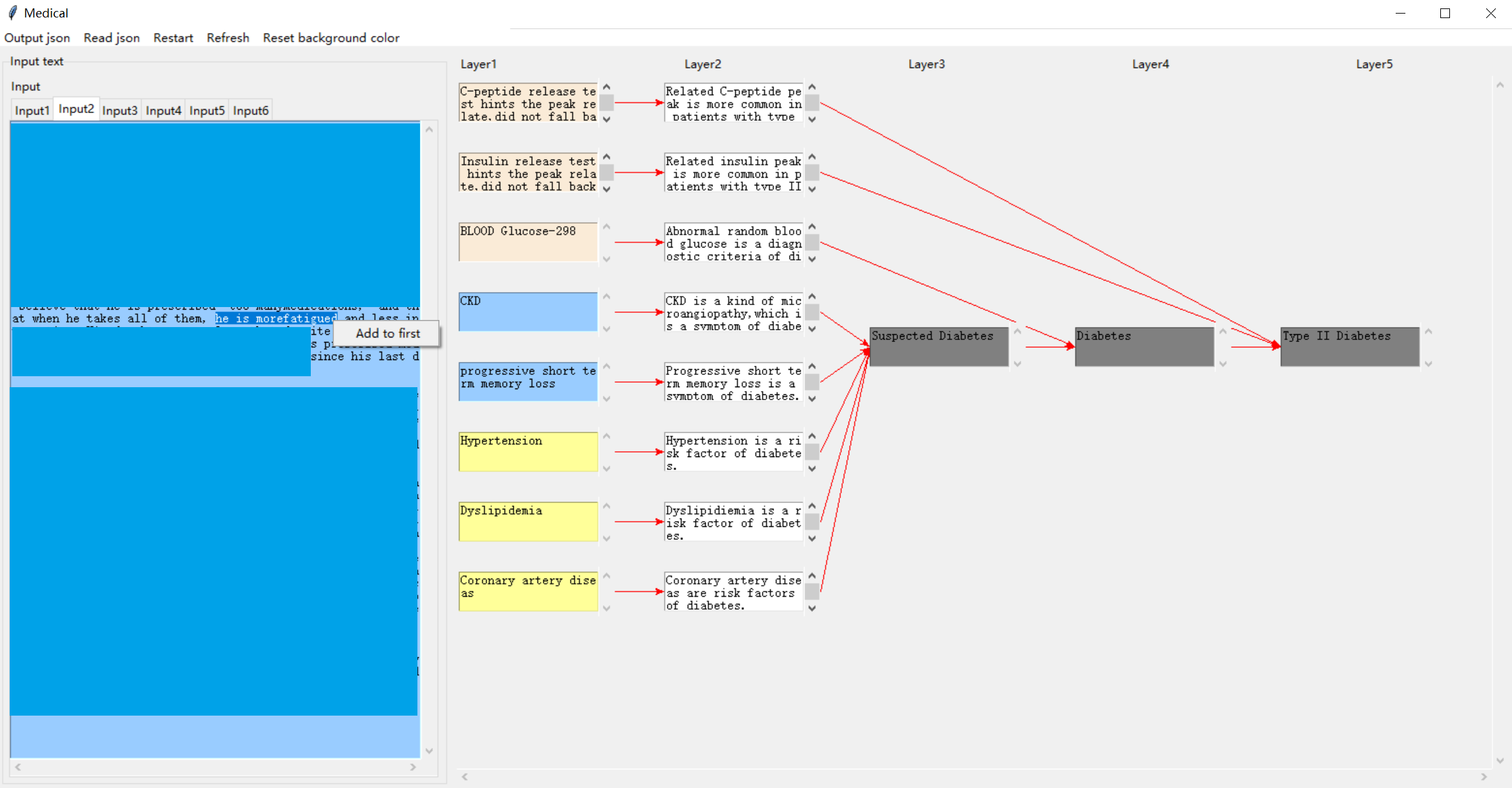
### Visual Description
## Diagram: Diabetes Risk Factor Pathway
### Overview
The image depicts a diagram illustrating potential pathways and risk factors leading to a diagnosis of Type II Diabetes. The diagram is structured as a multi-layered flow chart, starting with initial inputs (Layer 1) and progressing through intermediate stages (Layers 2-4) to the final diagnosis (Layer 5). The diagram is presented within a software interface, labeled "Medical" at the top-left corner, with menu options like "Output.json", "Read json", "Restart", "Reset background color", and "Input" tabs visible.
### Components/Axes
The diagram is organized into five vertical layers, labeled "Layer1" through "Layer5" at the top. Arrows indicate the flow of information or progression from one stage to the next. The diagram includes the following risk factors/conditions:
* **Layer 1 (Inputs):**
* C-peptide release test hints the peak release did not fall back
* Insulin release test hints the peak release did not fall back
* Blood Glucose=298
* CKD
* Progressive short term memory loss
* Hypertension
* Dyslipidemia
* Coronary artery disease
* **Layer 2 (Intermediate):**
* Related C-peptide peak is more common in patients with type II
* Related insulin peak is more common in patients with type II
* Abnormal random blood glucose is a diagnostic criteria of diabetes
* CKD is a kind of microangiopathy, which is a symptom of diabetes
* Progressive short term memory loss is a symptom of diabetes
* Hypertension is a risk factor of diabetes
* Dyslipidemia is a risk factor of diabetes
* Coronary artery disease are risk factors of diabetes
* **Layer 3:**
* Suspected Diabetes
* **Layer 4:**
* Diabetes
* **Layer 5:**
* Type II Diabetes
There is also a block of text on the left side of the diagram, partially obscured, containing the phrase "at when he takes all of them, and less in site. Add to first since his last d".
### Detailed Analysis or Content Details
The diagram illustrates a network of potential indicators and risk factors that can lead to a diagnosis of Type II Diabetes.
* **C-peptide/Insulin Release Tests:** Abnormal results in these tests (Layer 1) are linked to a higher prevalence in Type II Diabetes patients (Layer 2).
* **Blood Glucose:** A high blood glucose level (298) is identified as a diagnostic criterion for diabetes (Layer 2).
* **CKD (Chronic Kidney Disease):** CKD is presented as both a symptom and a cause of diabetes, specifically microangiopathy (Layer 2).
* **Progressive Short-Term Memory Loss:** This is identified as a symptom of diabetes (Layer 2).
* **Hypertension, Dyslipidemia, Coronary Artery Disease:** These are all listed as risk factors for diabetes (Layer 2).
* **Flow:** The diagram shows a convergence of these factors towards a "Suspected Diabetes" stage (Layer 3), then "Diabetes" (Layer 4), and ultimately "Type II Diabetes" (Layer 5).
The text on the left side is fragmented and difficult to interpret fully, but appears to relate to medication or treatment history.
### Key Observations
The diagram emphasizes the multi-faceted nature of Type II Diabetes, highlighting that it can be triggered by a combination of physiological indicators (blood glucose, hormone levels), pre-existing conditions (CKD, hypertension), and symptoms (memory loss). The diagram does not quantify the risk associated with each factor, but rather presents them as contributing elements in a complex pathway.
### Interpretation
This diagram serves as a visual aid for understanding the complex etiology of Type II Diabetes. It suggests that a diagnosis is rarely based on a single factor but rather a constellation of indicators and risk factors. The diagram's structure implies a probabilistic model, where the presence of multiple factors increases the likelihood of a diabetes diagnosis. The inclusion of both symptoms and risk factors suggests a bidirectional relationship, where diabetes can both cause and be caused by these conditions. The fragmented text on the left hints at the importance of patient history and medication in the diagnostic process. The diagram is likely used as a tool for medical professionals to assess patient risk and guide diagnostic testing.
</details>
Figure 8: Demonstration of our annotation tool.
### A.4 Access to DiReCT
Implementation code and annotation tool are available through https://github.com/wbw520/DiReCT. Data will be released through PhysioNet due to safety issues according to the license of MIMIC-IV (PhysioNet Credentialed Health Data License 1.5.0). We will use the same license for DiReCT. The download link will be accessible via GitHub. We confirm that this GitHub link and data link are always accessible. We confirm that we will bear all responsibility in case of violation of rights.
## Appendix B Implementation of Baseline Method
### B.1 Prompt Settings
Table 7: Prompt for narrowing-down module.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will review a clinical ’Note’ and your ’Response’ is to diagnose the disease that the patient have for this admission. |
| All possible disease options are in a list structure: {disease_option}. |
| Note that you can only choose one disease from the disease options and directly output the origin name of that disease. |
| Now, start to complete your task. |
| Don’t output any information other than your ’Response’. |
| ’Note’: |
| {note} |
| Your ’Response’: |
Table 8: Prompt for perception module.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will review a part of clinical "Note" from a patient. |
| The disease for which the patient was admitted to hospital this time is {disease}. |
| Your task is to extract the original text as confidence "Observations" that lead to {disease}. |
| Here are some premise for the diagnosis of this disease category. You can refer them for your task. Premise are: {premise} |
| Note that you also need to briefly provide the "Reason" for your extraction. |
| Note that both "Observations" and "Reason" should be string. |
| Note that your "Response" should be a list structure as following |
| : [["Observation", "Reason"], ……, ["Observation", "Reason"]] |
| Note that if you can’t find any "Observation" your "Response" should be: []. |
| Now, start to complete your task. |
| Note that you should not output any information other than your "Response". |
| "Note": |
| {note} |
| Note that you should not output any information other than your "Response". |
| Your "Response": |
Table 9: Prompt for reasoning module.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will receive a list of "Observations" from a clinical "Note". These "Observations" are possible support to diagnose {disease}. |
| Based on these "Observations", you need to diagnose the "Disease" from the following options: {disease_option}. |
| Here are some golden standards to discriminate diseases. You can refer them for your task. Golden standards are: {premise} |
| Note that you can only choose one "Disease" from the disease options and directly output the name in disease options. |
| Note that you also required to select the "Observations" that satisfy the golden standard to diagnose the "Disease" you choose. |
| Note that you also required to provide the "Reason" for your choice. |
| Note that your "Response" should be a list structure as following |
| :[["Observation", "Reason", "Disease"], ……, ["Observation", "Reason", "Disease"]] |
| Note that if you can’t find any "Observation" to support a disease option, your "Response" should be: None |
| Now, start to complete your task. |
| Note that you should not output any information other than your "Response". |
| "Observations": |
| {observation} |
| Note that you should not output any information other than your "Response". |
| Your "Response": |
In this section, we demonstrate the prompt we used for each module (From Table 7 - 9 for narrowing-down, perception, and reasoning module, respectively).
In Table 7, {disease_option} is the name for all disease categories, and {note} is the content for the whole clinical note. The response for the model is the name of a possible disease $\hat{i}$ .
In Table 8, {disease} is the disease category name predicted in narrowing-down. The content marked blue is the premise, which is only provided during the $k$ setting. In this module, {premise} is offered with all information in the knowledge graph. Different to narrowing-down, {note} is implemented for each clinical data $R=\{r\}$ and the outputs are combined together for $\hat{O}$ and $\hat{E}$ .
In Table 9, {disease} is the disease category name and {disease_option} is consisted by the children nodes $\{d_n\}_n$ . Similarly, the premise on the blue is only available for the $k$ setting. It provides the premise that are criteria for the diagnosis of each children node. {observation} is the extracted $\hat{O}$ in previous step. We provide all the prompts and the complete implementation code on GitHub.
### B.2 Details of Automatic Evaluation
The automatic evaluation is realized by LLama3 8B. We demonstrate the prompt for this implement in Table 10 (for observation) and Table 11 (for rationalization). Note that we do not use few-shot samples for the evaluation of observation. In Table 10, {gt_observation} and {pred_observation} are from model prediction and ground-truth. As this is a simple similarity comparison task to discriminate whether the model finds similar observations to humans, LLama3 itself have such ability. We do not strict to exactly match due to the difference in length of extracted raw text (as long as the observation expresses the same description). In Table 11, {gt_reasoning} and {pred_reasoning} are from model prediction and ground-truth. We require the rationale to be complete (content of the expression can be understood from the rationale alone) and meaningful; therefore, we provide five samples for this evaluation. We also provide all the prompts and the complete implementation code on GitHub.
Table 10: Prompt for evaluation of observation.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will receive two "Observations" extracted from a patient’s clinical note. |
| Your task is to discriminate whether they textually description is similar? |
| Note that "Response" should be one selection from "Yes" or "No". |
| Now, start to complete your task. |
| Don’t output any information other than your "Response". |
| "Observation 1": {gt_observation} |
| "Observation 2": {pred_observation} |
| Your "Response": |
Table 11: Prompt for evaluation of rationalization.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will receive two "Reasoning" for the explanation of why an observation cause a disease. |
| Your task is to discriminate whether they explain a similar medical diagnosis premise? |
| Note that "Response" should be one selection from "Yes" or "No". |
| Here are some samples: |
| Sample 1: |
| "Reasoning 1": Facial sagging is a classic symptom of stroke |
| "Reasoning 2": Indicates possible facial nerve palsy, a common symptom of stroke |
| "Response": Yes |
| Sample 2: |
| "Reasoning 1": Family history of Diabetes is an important factor |
| "Reasoning 2": Patient’s mother had a history of Diabetes, indicating a possible genetic predisposition to stroke |
| "Response": Yes |
| Sample 3: |
| "Reasoning 1": headache is one of the common symptoms of HTN |
| "Reasoning 2": Possible symptom of HTN |
| "Response": No |
| Sample 4: |
| "Reasoning 1": Acute bleeding is one of the typical symptoms of hemorrhagic stroke |
| "Reasoning 2": The presence of high-density areas on Non-contrast CT Scan is a golden standard for Hemorrhagic Stroke |
| "Response": No |
| Sample 5: |
| "Reasoning 1": Loss of strength on one side of the body, especially when compared to the other side, is a common sign of stroke |
| "Reasoning 2": Supports ischemic stroke diagnosis |
| "Response": No |
| Now, start to complete your task. |
| Don’t output any information other than your "Response". |
| "Reasoning 1": {gt_reasoning} |
| "Reasoning 2": {pred_reasoning} |
| Your "Response": |
### B.3 Prediction Samples
Figure 9 and 10 shows two sample generated by GPT-4. The ground-truth PDD of the input clinical note is Gastroesophageal Reflux Disease (GERD) and Heart Failure (HF). In these figure, purple, orange, and red indicate explanations only in the ground truth, only in prediction, and common in both, respectively; therefore, red is a successful prediction of an explanation, while purple and orange are a false negative and false positive.
<details>
<summary>x8.png Details</summary>
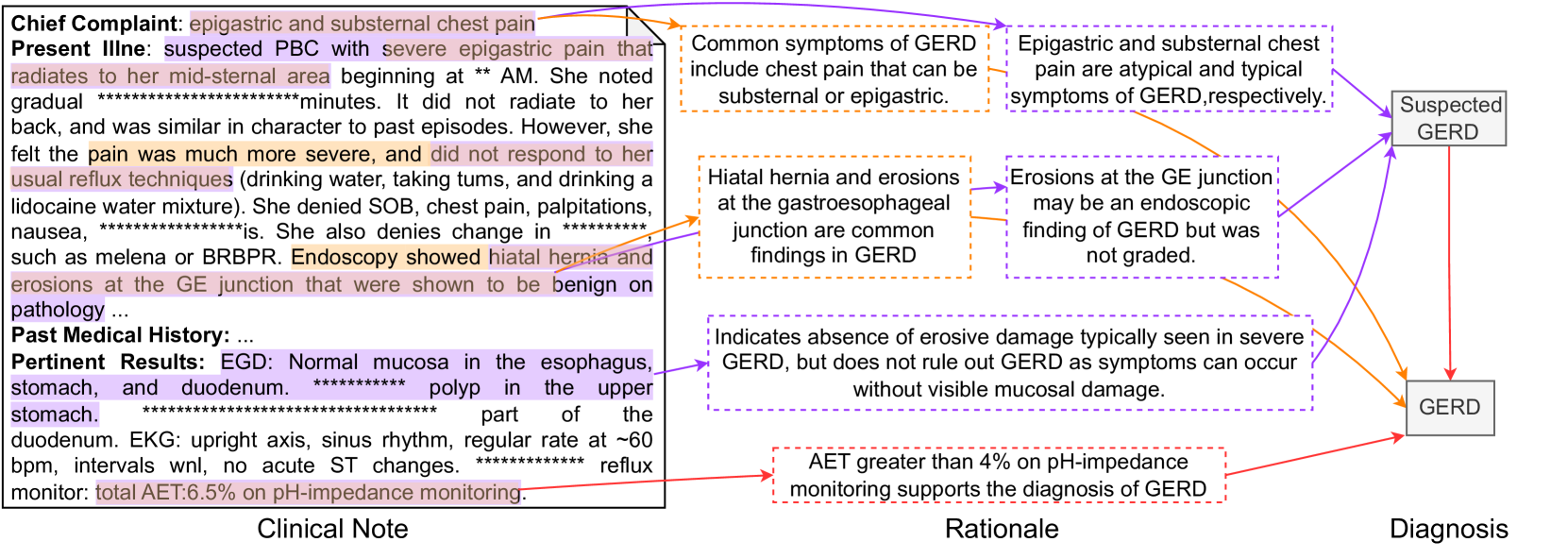
### Visual Description
\n
## Flowchart: GERD Diagnostic Pathway
### Overview
This image presents a flowchart illustrating the diagnostic pathway for suspected Gastroesophageal Reflux Disease (GERD). It links clinical notes, rationale, and diagnosis, outlining the process from initial complaint to final diagnosis. The flowchart uses boxes to represent stages and arrows to indicate the flow of information.
### Components/Axes
The flowchart is divided into three main sections: "Clinical Note" (left), "Rationale" (center), and "Diagnosis" (right). Each section contains text boxes with information. Arrows connect these boxes, indicating the progression of the diagnostic process.
### Detailed Analysis or Content Details
**Clinical Note:**
* **Chief Complaint:** epigastric and substernal chest pain
* **Present Illness:** suspected PBC with severe epigastric pain that radiates to her mid-sternal area beginning at approximately 2 AM. She noted gradual pain over ~minutes. It did not radiate to her back, and was similar in character to past episodes. However, she felt the pain was much more severe, and did not respond to her usual reflux techniques (drinking water, taking turns, and drinking a lidocaine water mixture). She denied SOB, chest pain, palpitations, nausea, and changes in bowel habits such as melena or BRBPR. Endoscopy showed hiatal hernia and erosions at the GE junction that were shown to be benign on pathology.
* **Past Medical History:** ...
* **Pertinent Results:** EGD: Normal mucosa in the esophagus, stomach, and duodenum. Polyp in the upper stomach. Part of the duodenum. EKG: upright axis, sinus rhythm, regular rate at ~60 bpm, intervals w/n, no acute ST changes. Reflux monitor: total AET 6.5% on pH-impedance monitoring.
**Rationale:**
* Common symptoms of GERD include chest pain that can be substernal or epigastric.
* Epigastric and substernal chest pain are atypical and typical symptoms of GERD respectively.
* Hiatal hernia and erosions at the gastroesophageal junction are common findings in GERD.
* Erosions at the GE junction may be an endoscopic finding of GERD but was not graded.
* Indicates absence of erosive damage typically seen in severe GERD, but does not rule out GERD as symptoms can occur without visible mucosal damage.
* AET greater than 4% on pH-impedance monitoring supports the diagnosis of GERD.
**Diagnosis:**
* Suspected GERD (initial stage)
* GERD (final diagnosis)
The arrows indicate the following flow:
1. Clinical Note -> Rationale (Common Symptoms) -> Suspected GERD
2. Clinical Note -> Rationale (Hiatal Hernia/Erosions) -> Suspected GERD
3. Clinical Note -> Rationale (Erosions at GE Junction) -> Suspected GERD
4. Clinical Note -> Rationale (Absence of Erosive Damage) -> Suspected GERD
5. Clinical Note -> Rationale (AET > 4%) -> GERD
### Key Observations
The flowchart highlights that GERD diagnosis isn't solely based on the presence of erosions. Atypical symptoms, hiatal hernia, and pH-impedance monitoring results (AET > 4%) play a crucial role. The progression from "Suspected GERD" to "GERD" is dependent on the rationale provided.
### Interpretation
This flowchart demonstrates a clinical decision-making process for GERD. It emphasizes that GERD can be diagnosed even in the absence of significant erosive damage, relying on a combination of symptom presentation, endoscopic findings (like hiatal hernia), and physiological testing (pH-impedance monitoring). The AET value of 6.5% (from the clinical note) is a key factor supporting the final diagnosis of GERD. The flowchart is a simplified representation of a complex diagnostic process, but it effectively illustrates the key considerations for clinicians. The use of "approximately" (~), and "within" (w/n) indicates uncertainty in the values. The repeated asterisks (********) likely represent redacted patient information.
</details>
Figure 9: An example prediction for a clinical note with PDD of GERD by GPT-4
<details>
<summary>x9.png Details</summary>
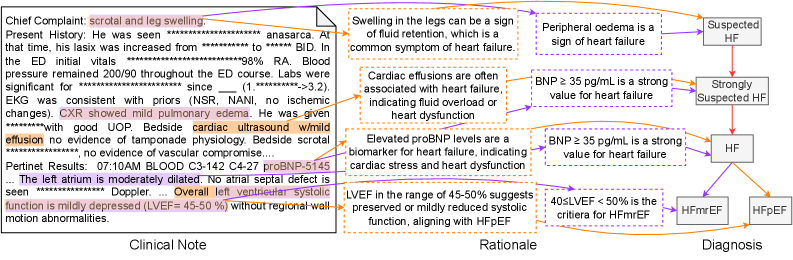
### Visual Description
\n
## Diagram: Heart Failure Diagnostic Pathway
### Overview
This diagram illustrates a clinical pathway for diagnosing heart failure (HF), linking clinical notes, rationale, and potential diagnoses. It presents a flow of information from patient presentation to diagnostic considerations, with specific biomarkers and clinical findings guiding the diagnostic process. The diagram is divided into three main sections: "Clinical Note" (left), "Rationale" (center), and "Diagnosis" (right).
### Components/Axes
The diagram consists of text blocks connected by arrows indicating a flow of reasoning. The sections are labeled "Clinical Note", "Rationale", and "Diagnosis" at the bottom. The diagram uses color-coding to differentiate diagnostic outcomes: yellow for "Suspected HF", orange for "Strongly Suspected HF", and purple for "HF" (further categorized into HfmrEF and HfPEf).
### Detailed Analysis or Content Details
**Clinical Note (Left Section):**
The clinical note section contains a block of text with the following information:
* **Chief Complaint:** scrotal and leg swelling.
* **Present History:** He was seen anasarca. At that time, his lasix was increased from ***** to ***** BID. In the ED initial vitals *****% RA. Blood pressure remained 200/90 throughout the ED course. Labs were significant for ***** since (1, *****->3.2). EKG was consistent with priors (NSR, NANI, no ischemic changes). CXR showed mild pulmonary edema. He was given ***** with good UOP. Bedside cardiac ultrasound w/mild effusion no evidence of tamponade physiology. Bedside scrotal *****, no evidence of vascular compromise.
* **Pertinent Results:** 07:10AM BLOOD C3-142 C4-27 proBNP-5145. The left atrium is moderately dilated. No atrial septal defect is seen. Doppler... Overall left ventricular systolic function is mildly depressed (LVEF = 45-50%) without regional wall motion abnormalities.
**Rationale (Center Section):**
* Swelling in the legs can be a sign of fluid retention, which is a common symptom of heart failure.
* Cardiac effusions are often associated with heart failure, indicating fluid overload or heart dysfunction.
* Elevated proBNP levels are a biomarker for heart failure, indicating cardiac stress and heart dysfunction.
* LVEF in the range of 45-50% suggests preserved or mildly reduced systolic function, aligning with HFpEF.
**Diagnosis (Right Section):**
* **BNP ≥ 35 pg/mL is a strong value for heart failure** (connected to "Strongly Suspected HF").
* **BNP ≥ 35 pg/mL is a strong value for heart failure** (connected to "HF").
* **40≤LVEF <50% is the criteria for HfmrEF** (connected to "HF").
* **HF** branches into two diagnoses: **HfmrEF** (Heart Failure with mildly Reduced Ejection Fraction) and **HfPEf** (Heart Failure with Preserved Ejection Fraction).
* **Peripheral edema is a sign of heart failure** (connected to "Suspected HF").
**Color Coding & Arrows:**
* Yellow arrows lead from the rationale to "Suspected HF".
* Orange arrows lead from the rationale to "Strongly Suspected HF".
* Purple arrows lead from the rationale to "HF", which then branches to HfmrEF and HfPEf.
### Key Observations
* The diagram emphasizes the importance of clinical findings (edema, effusion), biomarkers (proBNP), and LVEF in the diagnostic process.
* The proBNP level of 5145 is highlighted as a significant finding.
* The LVEF range of 45-50% is specifically linked to HFpEF.
* The diagram shows a progression from initial suspicion to more definitive diagnoses based on accumulating evidence.
### Interpretation
This diagram represents a simplified clinical decision-making process for heart failure. It demonstrates how a combination of subjective clinical observations (swelling) and objective measurements (proBNP, LVEF) are used to arrive at a diagnosis. The branching pathways suggest that the diagnosis is not always straightforward and depends on the specific clinical presentation and test results. The color-coding visually represents the level of certainty in the diagnosis, with yellow indicating initial suspicion and purple indicating a more confident diagnosis. The diagram highlights the importance of considering both systolic and diastolic function in the evaluation of heart failure, as evidenced by the distinction between HfmrEF and HfPEf. The redacted portions of the clinical note suggest sensitive patient information is being protected. The diagram is a useful tool for clinicians to understand the diagnostic pathway and guide their clinical decision-making.
</details>
Figure 10: An example prediction for a clinical note with PDD of HF by GPT-4
In Figure 9, we can observe that GPT-4 can find the key observation for the diagnosis of GERD, which is consistent with human in both observation and rationale. However, it still lacks the ability to identify all observations and establish accurate relationships for diseases. In Figure 10, the model’s predictions do not align well with those of a human doctor. Key observations, such as the relationships between BNP and LVEF, are incorrectly identified, leading to a final misdiagnosis.
### B.4 Experiments for No Extra Knowledge
Table 12: Prompt for $D^⋆$ setting.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will review a clinical ’Note’ and your ’Response’ is to diagnose the disease that the patient have for this admission. |
| All possible disease options are in a list structure: {disease_options}. |
| Note that you can only choose one disease from the disease options and directly output the origin name of that disease. |
| Now, start to complete your task. |
| Don’t output any information other than your ’Response’. |
| ’Note’: |
| {note} |
| Your ’Response’: |
Table 13: Prompt for no knowledge setting.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will review a clinical ’Note’ and your ’Response’ is to diagnose the disease that the patient have for this admission. |
| Note that you can only give one disease name and directly output the name of that "Disease". |
| Now, start to complete your task. |
| Don’t output any information other than your ’Response’. |
| ’Note’: |
| {note} |
| Your ’Response’: |
We demonstrate the prompt used for $D^⋆$ and no knowledge settings in Table 12 and Table 13, respectively. {note} is the text of whole clinical note and {note} in Table 12 is the name of all leaf node $D^⋆$ .
### B.5 Experimental Settings
All experiments are implemented with a temperature value of 0. All close sourced models are implemented in a local server with 4 NVIDIA A100 GPU.
## Appendix C Failed Attempts on DiReCT
In this section, we discuss some unsuccessful attempts during the experiments.
Extract observation from the whole clinical note. We try to diagnose the disease and extract observation, and the corresponding rationale using the prompt shown in Table 14. The {note} is offered by the whole content in the clinical note. We find that even though the model can make the correct diagnosis, only a few observations can be extracted (no more than 4), which decreases the completeness and faithfulness.
Table 14: Prompt for extracting observation in one step.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will review a clinical ’Note’, and your ’Response’ is to diagnose the disease that the patient has for this admission. |
| All possible disease options are in a list structure: {disease_options}. |
| Note that you can only choose one disease from the disease options and directly output the origin name of that disease. |
| Note that you also need to extract original text as confidence "Observations" that lead to the "Disease" you selected. |
| Note that you should extract all necessary "Observation". |
| Note that you also need to briefly provide the "Reason" for your extraction. |
| Note that both "Observations" and "Reason" should be string. |
| Note that your "Response" should be a list structure as following |
| :[["Observation", "Reason", "Disease"], ……, ["Observation", "Reason", "Disease"]] |
| Now, start to complete your task. |
| Don’t output any information other than your ’Response’. |
| ’Note’ |
| : {note} |
| Your ’Response’: |
End-to-End prediction. We also try to output the whole reasoning process in one step (without iteration) when given observations. We show our prompt in Table 15. We find that using such a prompt model can not correctly recognize the relation between observation, rationale, and diagnosis.
Table 15: Prompt for extracting observation in one step.
| Input Prompt |
| --- |
| Suppose you are one of the greatest AI scientists and medical expert. Let us think step by step. |
| You will receive a list of "Observations" from a clinical "Note" for the diagnosis of stroke. |
| Here is the diagnostic route of stroke in a tree structure: |
| -Suspected Stroke |
| -Hemorrhagic Stroke |
| -Ischemic Stroke |
| Here are some premise for the diagnosis of this disease. You can refer them for your task. Premise are: {premise} |
| Based on these "Observations", starting from the root disease, your target is to diagnose one of the leaf disease. |
| Note that you also required to provide the "Reason" for your reasoning. |
| Note that your "Response" should be a list structure as following |
| :[["Observation", "Reason", "Disease"], ……, ["Observation", "Reason", "Disease"]] |
| Note that if you can’t find any "Observation" to support a disease option, your "Response" should be: None |
| Now, start to complete your task. |
| Note that you should not output any information other than your "Response". |
| "Observations": |
| {observation} |
| Note that you should not output any information other than your "Response". |
| Your "Response": |
## Appendix D Ethical Considerations
Utilizing real-world EHRs, even in a de-identified form, poses inherent risks to patient privacy. Therefore, it is essential to implement rigorous data protection and privacy measures to safeguard sensitive information, in accordance with regulations such as HIPAA. We strictly adhere to the Data Use Agreement of the MIMIC dataset, ensuring that the data is not shared with any third parties. All experiments are implement on a private server. The access to GPT is also a private version.
AI models are susceptible to replicating and even intensifying the biases inherent in their training data. These biases, if not addressed, can have profound implications, particularly in sensitive domains such as healthcare. Unconscious biases in healthcare systems can result in significant disparities in the quality of care and health outcomes among different demographic groups. Therefore, it is imperative to rigorously examine AI models for potential biases and implement robust mechanisms for ongoing monitoring and evaluation. This involves analyzing the model’s performance across various demographic groups, identifying any disparities, and making necessary adjustments to ensure equitable treatment for all. Continual vigilance and proactive measures are essential to mitigate the risk of biased decision-making and to uphold the principles of fairness and justice in AI-driven healthcare solutions.