TECHNICAL ASSET FINGERPRINT
192c5c9dc98d960eb6f13aef
Click to view fullscreen
Press ESC or click to close
FOUND IN PAPERS
EXPERT: healer-alpha-free VERSION 1
RUNTIME: free/openrouter/healer-alpha
INTEL_VERIFIED
## Medical Case Analysis Diagram: Clinical Note to Stroke Diagnosis
### Overview
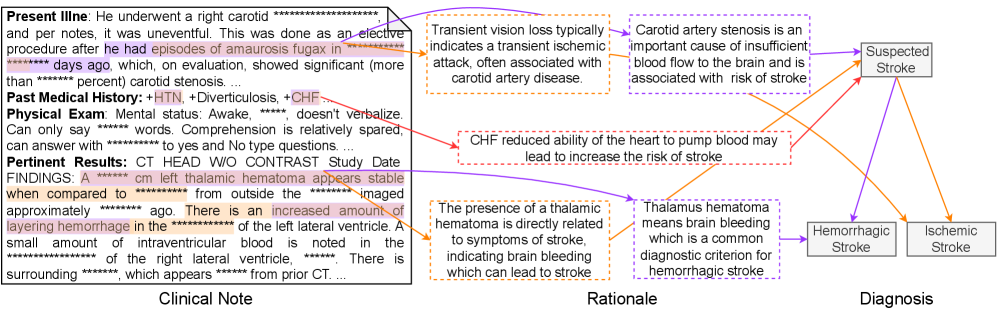
This image is a structured medical case analysis diagram that connects a de-identified clinical note to diagnostic reasoning. It visually maps specific findings from a patient's clinical presentation to their pathophysiological rationale and final diagnostic classification. The diagram is divided into three primary vertical sections: **Clinical Note** (left), **Rationale** (center), and **Diagnosis** (right). Color-coded arrows create explicit links between clinical data points, their medical explanations, and the resulting diagnostic conclusions.
### Components/Axes
The diagram is organized into three distinct regions:
1. **Clinical Note (Left Section):** Contains transcribed text from a patient's medical record, divided into four subsections:
* **Present Illness:** Describes a right carotid procedure, amaurosis fugax, and significant carotid stenosis.
* **Past Medical History:** Lists comorbidities: HTN (Hypertension), Diverticulosis, and CHF (Congestive Heart Failure).
* **Physical Exam:** Notes mental status, verbal limitations, and comprehension.
* **Pertinent Results:** Details CT head findings, including a stable left thalamic hematoma, increased layering hemorrhage, and a small amount of intraventricular blood.
* *Note: Several specific values (e.g., days ago, percent stenosis, hematoma size in cm, exact timeframes) are redacted with asterisks (`***`).*
2. **Rationale (Center Section):** Contains four explanatory text boxes that provide the medical reasoning linking clinical findings to stroke risk. Each box is connected by a colored arrow to the relevant part of the Clinical Note.
* **Top (Purple Arrow):** "Transient vision loss typically indicates a transient ischemic attack, often associated with carotid artery disease." / "Carotid artery stenosis is an important cause of insufficient blood flow to the brain and is associated with risk of stroke."
* **Middle (Red Arrow):** "CHF reduced ability of the heart to pump blood may lead to increase the risk of stroke."
* **Bottom (Orange Arrow):** "The presence of a thalamic hematoma is directly related to symptoms of stroke, indicating brain bleeding which can lead to stroke." / "Thalamus hematoma means brain bleeding which is a common diagnostic criterion for hemorrhagic stroke."
3. **Diagnosis (Right Section):** A flowchart that culminates in a diagnostic conclusion.
* A central box labeled **"Suspected Stroke"** is the convergence point for all rationale arrows.
* From "Suspected Stroke," two arrows point to final diagnostic categories:
* **"Hemorrhagic Stroke"** (connected via an orange arrow originating from the thalamic hematoma rationale).
* **"Ischemic Stroke"** (connected via a purple arrow originating from the carotid stenosis rationale).
### Detailed Analysis
**Textual Transcription & Linkages:**
* **Clinical Note - Present Illness:** "He underwent a right carotid ************ and notes this was done as an elective procedure after he had episodes of amaurosis fugax in ************ days ago, which on evaluation, showed significant (more than ************ percent) carotid stenosis..."
* **Linked Rationale (Purple Arrow):** Connects "amaurosis fugax" and "carotid stenosis" to the rationale explaining transient ischemic attack (TIA) and stroke risk from insufficient blood flow.
* **Clinical Note - Past Medical History:** "+HTN, +Diverticulosis, +CHF"
* **Linked Rationale (Red Arrow):** Connects "+CHF" to the rationale explaining how reduced cardiac output increases stroke risk.
* **Clinical Note - Pertinent Results:** "FINDINGS: A ************ cm left thalamic hematoma appears stable when compared to ************ from outside the ************ imaged approximately ************ ago. There is an increased amount of layering hemorrhage in the ************ of the left lateral ventricle. A small amount of intraventricular blood is noted in the ************ of the right lateral ventricle. ************. There is surrounding ************, which appears ************ from prior CT..."
* **Linked Rationale (Orange Arrow):** Connects "left thalamic hematoma" and "layering hemorrhage" to the rationale explaining that brain bleeding (hemorrhage) is a diagnostic criterion for hemorrhagic stroke.
**Diagnostic Flowchart Logic:**
The diagram presents a multi-factorial diagnostic assessment:
1. **Evidence for Ischemic Stroke:** The history of amaurosis fugax (a TIA symptom) and significant carotid stenosis (purple pathway) points toward an ischemic etiology (blockage).
2. **Evidence for Hemorrhagic Stroke:** The CT finding of a thalamic hematoma with intraventricular extension (orange pathway) is direct evidence of brain bleeding, defining a hemorrhagic stroke.
3. **Contributing Risk Factor:** The presence of CHF (red pathway) is noted as a general risk factor that increases the likelihood of stroke but does not specify the type.
The final diagnosis is therefore not singular but presents two concurrent possibilities ("Suspected Stroke" branching to both types), reflecting the complex clinical picture where evidence for both ischemic and hemorrhagic pathology exists.
### Key Observations
1. **Dual Pathology:** The most significant observation is the simultaneous presentation of clinical evidence strongly suggestive of *both* ischemic (carotid disease) and hemorrhagic (thalamic bleed) stroke mechanisms.
2. **Spatial Grounding of Arrows:**
* The **purple arrow** originates from the "Present Illness" text block (top-left of Clinical Note) and flows to the top Rationale box, then to "Suspected Stroke," and finally to "Ischemic Stroke."
* The **red arrow** originates from the "Past Medical History" line (middle-left) and flows to the middle Rationale box, then to "Suspected Stroke."
* The **orange arrow** originates from the "Pertinent Results" text block (bottom-left) and flows to the bottom Rationale box, then to "Suspected Stroke," and finally to "Hemorrhagic Stroke."
3. **Redacted Information:** Key quantitative data (time intervals, stenosis percentage, hematoma dimensions) is obscured, limiting precise clinical staging but not the logical flow of the diagnostic reasoning.
4. **Anatomical Specificity:** The hemorrhage is localized to the left thalamus with extension into the ventricles, a critical detail for prognosis and treatment planning.
### Interpretation
This diagram is a powerful tool for **clinical reasoning visualization**. It demonstrates how a clinician synthesizes disparate data points—a symptom (amaurosis fugax), a chronic condition (carotid stenosis), a comorbidity (CHF), and an acute imaging finding (thalamic hematoma)—into a coherent diagnostic hypothesis.
The data suggests a patient with significant vascular disease (carotid stenosis) who has now presented with an acute intracranial hemorrhage. The "interpretation" is that this is a complex case where the stroke type is ambiguous based on initial presentation alone. The diagram argues that while the hemorrhage is confirmed on imaging (making hemorrhagic stroke a certainty), the underlying etiology could also involve ischemic mechanisms (e.g., hemorrhagic transformation of an ischemic infarct, or a primary bleed in a patient with concomitant severe atherosclerotic disease).
The inclusion of CHF as a separate, converging risk factor highlights the importance of considering systemic conditions that exacerbate cerebrovascular risk. Ultimately, the diagram does not provide a single answer but maps the **diagnostic uncertainty** and the **competing pathophysiologies** that must be considered in management. It serves as a template for understanding how to trace clinical evidence to its mechanistic rationale and then to a differential diagnosis.
DECODING INTELLIGENCE...