TECHNICAL ASSET FINGERPRINT
7d877cd87f618781986734f1
Click to view fullscreen
Press ESC or click to close
FOUND IN PAPERS
EXPERT: healer-alpha-free VERSION 1
RUNTIME: free/openrouter/healer-alpha
INTEL_VERIFIED
## Clinical Document: Heart Failure Diagnostic Pathway
### Overview
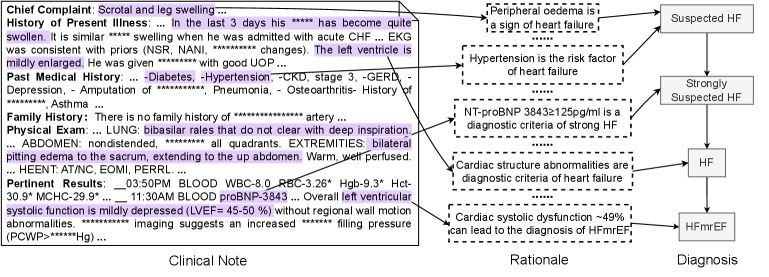
The image is a composite technical diagram illustrating the diagnostic reasoning process for a patient presenting with symptoms suggestive of heart failure. It integrates a clinical note (left), a rationale section linking findings to diagnostic criteria (center), and a diagnostic flowchart (right). The document demonstrates how specific patient data points map to established medical criteria to arrive at a diagnosis of Heart Failure with mildly reduced Ejection Fraction (HFmrEF).
### Components/Axes
The image is segmented into three primary vertical regions:
1. **Left Region: Clinical Note**
* **Structure:** A structured medical note with labeled sections.
* **Sections & Content:**
* **Chief Complaint:** "Scrotal and leg swelling ..."
* **History of Present Illness:** Describes 3 days of worsening swelling, similar to a prior admission for acute CHF. Notes consistent EKG, mildly enlarged left ventricle, and good response to IV diuretics (I/V diuretics).
* **Past Medical History:** Lists Diabetes, Hypertension, CKD (stage 3), GERD, history of [REDACTED] embolization, Pneumonia, Osteoarthritis, Asthma.
* **Family History:** "There is no family history of ... artery ..."
* **Physical Exam:**
* LUNG: "bibasilar rales that do not clear with deep inspiration ..."
* ABDOMEN: "soft, nontender, ... all quadrants."
* EXTREMITIES: "bilateral pitting edema to the sacrum extending to the low abdomen. Warm. Well perfused."
* CV: "RRR, no EOMI, PERRLA."
* **Recent Results:**
* "1:50PM BLOOD WBC-8.0 *RBC-3.26* Hgb-9.3* Hct-30.9* MCHC-29.9* 11:30AM BLOOD proBNP-3843 ..."
* "Overall left ventricular systolic function is mildly depressed (LVEF= 45-50 %) without regional wall motion abnormalities. ... imaging suggests an increased ... filling pressure (PCWP=... mmHg)."
2. **Center Region: Rationale**
* **Structure:** A series of text boxes with arrows pointing from specific findings in the Clinical Note to explanatory diagnostic statements.
* **Boxes & Connections (from top to bottom):**
* Arrow from "Scrotal and leg swelling" and "bilateral pitting edema..." → Box: "Peripheral edema is a sign of heart failure."
* Arrow from "Hypertension" in Past Medical History → Box: "Hypertension is the risk factor of heart failure."
* Arrow from "proBNP-3843" in Recent Results → Box: "NT-proBNP 3843≥125pg/ml is a diagnostic criteria of strong HF."
* Arrow from "mildly enlarged" left ventricle and "increased ... filling pressure" → Box: "Cardiac structure abnormalities are diagnostic criteria of heart failure."
* Arrow from "LVEF= 45-50 %" → Box: "Cardiac systolic dysfunction ~49% can lead to the diagnosis of HFmrEF."
3. **Right Region: Diagnosis Flowchart**
* **Structure:** A vertical flowchart with rectangular boxes connected by downward-pointing arrows.
* **Flow:** Suspected HF → Strongly Suspected HF → HF → HFmrEF.
### Detailed Analysis
**Clinical Data Extraction:**
* **Key Lab Value:** NT-proBNP = 3843 pg/ml. The rationale explicitly states this meets the diagnostic criterion of ≥125 pg/ml for "strong HF."
* **Echocardiogram Finding:** Left Ventricular Ejection Fraction (LVEF) is 45-50%. The rationale interprets this as "~49%" systolic dysfunction, leading to the specific diagnosis of HFmrEF (typically defined as LVEF 41-49%).
* **Supporting Signs:** Peripheral edema (scrotal, leg, sacral pitting edema), bibasilar rales, history of hypertension, and evidence of increased cardiac filling pressure (PCWP value redacted).
* **Redacted Information:** Several terms are obscured with asterisks (`...`), including specific medications, a prior embolization site, and the exact PCWP value.
**Diagnostic Logic Flow:**
The rationale section creates a direct, evidence-based link between patient findings and diagnostic rules:
1. **Symptom (Edema)** → Sign of HF.
2. **Risk Factor (Hypertension)** → Predisposes to HF.
3. **Biomarker (NT-proBNP 3843)** → Meets quantitative criterion for strong HF.
4. **Structural Abnormality (Enlarged LV, increased filling pressure)** → Meets structural criterion for HF.
5. **Functional Abnormality (LVEF 45-50%)** → Specifies the subtype as HFmrEF.
This cumulative evidence progresses the diagnosis from "Suspected" to "Strongly Suspected," confirms "HF," and finally specifies "HFmrEF."
### Key Observations
1. **Quantitative Thresholds:** The document explicitly references diagnostic thresholds (NT-proBNP ≥125 pg/ml, LVEF ~49% for HFmrEF), showing a criteria-based diagnostic approach.
2. **Multi-Factorial Diagnosis:** The diagnosis is not based on a single finding but on the convergence of symptoms (edema), signs (rales), risk factors (HTN), biomarkers (BNP), and imaging (echo).
3. **Specificity in Classification:** The pathway doesn't stop at a general "Heart Failure" diagnosis but uses the LVEF value to specify the subtype (HFmrEF), which has different therapeutic implications.
4. **Data Gaps:** The redacted information (PCWP value, specific medications, embolization history) represents missing data that would be relevant for a complete clinical picture but is not essential for the demonstrated diagnostic logic.
### Interpretation
This diagram serves as a pedagogical or clinical decision-support tool that visualizes the **Peircean abductive reasoning** common in medicine: starting from an observation (symptoms/signs), applying known medical rules (diagnostic criteria), and inferring the most plausible explanation (HFmrEF diagnosis).
* **What the Data Suggests:** The patient's clinical profile is a classic presentation of heart failure, specifically the mildly reduced ejection fraction subtype. The elevated NT-proBNP is a strong objective indicator of cardiac stress, corroborating the subjective symptoms and physical exam findings.
* **How Elements Relate:** The three panels form a logical chain: **Evidence (Note)** → **Reasoning (Rationale)** → **Conclusion (Diagnosis Flowchart)**. The arrows in the Rationale section are critical, as they explicitly map raw data to medical knowledge, transforming information into actionable diagnosis.
* **Notable Patterns/Anomalies:** The pattern is one of **convergent validity**—multiple independent lines of evidence point to the same conclusion. There are no apparent anomalies or contradictory findings in the presented data. The LVEF of 45-50% is the key data point that refines the diagnosis from generic HF to the specific HFmrEF category, highlighting the importance of precise measurement in guiding classification and subsequent treatment.
DECODING INTELLIGENCE...