TECHNICAL ASSET FINGERPRINT
c4b0a1228b3c644d0eafd157
Click to view fullscreen
Press ESC or click to close
FOUND IN PAPERS
EXPERT: healer-alpha-free VERSION 1
RUNTIME: free/openrouter/healer-alpha
INTEL_VERIFIED
## Medical Case Analysis Diagram: GERD Diagnosis Pathway
### Overview
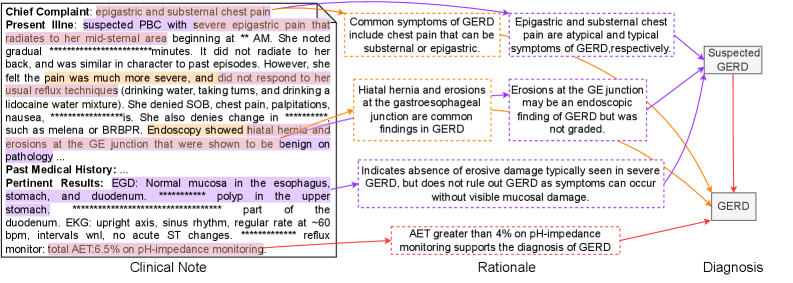
The image is a structured medical case analysis diagram that presents a patient's clinical information, the diagnostic rationale, and the final diagnosis. It is organized into three distinct vertical sections: **Clinical Note** (left), **Rationale** (center), and **Diagnosis** (right). The diagram uses text boxes and directional arrows to illustrate the logical flow from patient symptoms and test results to a diagnosis of Gastroesophageal Reflux Disease (GERD).
### Components/Axes
The diagram is segmented into three primary regions:
1. **Clinical Note (Left Section):** Contains the raw patient data.
* **Chief Complaint:** "epigastric and substernal chest pain"
* **Present Illness:** A detailed narrative describing the onset, character, radiation, associated symptoms, and relevant test results. Key findings include:
* Pain described as "severe" and "burning," radiating to the mid-sternal area.
* Symptoms worsened with "certain triggers (drinking water, taking turns, and drinking a licorice water mixture)."
* Denial of SOB, chest pain, palpitations, nausea, `*********`.
* Denial of melena or BRBPR.
* **Endoscopy Result:** "showed hiatal hernia and erosions at the GE junction that were shown to be benign on pathology."
* **Past Medical History:** `*********`
* **Past Results:**
* **EGD:** "Normal mucosa in the esophagus, stomach, and duodenum. ********* polyp in the upper part of the duodenum."
* **EKG:** "upright axis, sinus rhythm, regular rate at ~60bpm, intervals wnl, no acute ST changes."
* **Reflux Monitor:** "total AET 5.5% on pH-impedance monitoring"
2. **Rationale (Center Section):** A flowchart of explanatory boxes that interpret the clinical data. Each box is connected by arrows to the relevant part of the Clinical Note and to the final diagnosis.
* **Box 1 (Top):** "Common symptoms of GERD include chest pain that can be substernal or epigastric."
* **Box 2 (Top-Right):** "Epigastric and substernal chest pain are atypical and typical symptoms of GERD respectively."
* **Box 3 (Middle-Left):** "Hiatal hernia and erosions at the gastroesophageal junction are common findings in GERD."
* **Box 4 (Middle-Right):** "Erosions at the GE junction may be an endoscopic finding of GERD but was not graded."
* **Box 5 (Bottom-Left):** "Indicates absence of erosive damage typically seen in severe GERD, but does not rule out GERD as symptoms can occur without visible mucosal damage."
* **Box 6 (Bottom-Right):** "AET greater than 4% on pH-impedance monitoring supports the diagnosis of GERD."
3. **Diagnosis (Right Section):** A single box stating the final conclusion.
* **Diagnosis:** "GERD"
* A preceding box labeled "Suspected GERD" is also present, with arrows leading from the Rationale section to it, and then to the final "GERD" box.
### Detailed Analysis
* **Data Flow & Connections:**
* The **Chief Complaint** and **Present Illness** narrative are linked via arrows to Rationale Boxes 1, 2, 3, and 4.
* The **Endoscopy Result** ("hiatal hernia and erosions") is specifically linked to Rationale Boxes 3 and 4.
* The **EGD Result** ("Normal mucosa") is linked to Rationale Box 5.
* The **Reflux Monitor Result** ("AET 5.5%") is linked to Rationale Box 6.
* All Rationale Boxes (1-6) have arrows pointing to the "Suspected GERD" box, which then points to the final "GERD" diagnosis.
* **Key Data Points Extracted:**
* **Symptom Onset:** `** AM` (specific time redacted).
* **Symptom Duration:** `********* minutes` (specific duration redacted).
* **Endoscopic Findings:** Hiatal hernia and erosions at the gastroesophageal (GE) junction. Pathology showed these were benign.
* **EGD Findings:** Normal mucosa in esophagus, stomach, and duodenum; a polyp in the upper duodenum.
* **EKG Findings:** Normal sinus rhythm at ~60 bpm, no acute changes.
* **pH-Impedance Monitoring Result:** Total Acid Exposure Time (AET) = 5.5%.
### Key Observations
1. **Contradictory Evidence:** The diagram highlights a key diagnostic tension. The endoscopy showed erosions (a sign of erosive GERD), but the EGD report states "Normal mucosa." The rationale (Box 5) reconciles this by noting that non-erosive reflux disease (NERD) exists.
2. **Objective Metric:** The pH-impedance monitoring provides an objective, quantitative measure (AET 5.5%) that exceeds the diagnostic threshold (>4%), strongly supporting the GERD diagnosis.
3. **Symptom Correlation:** The rationale explicitly connects the patient's specific symptoms (epigastric/substernal pain, trigger-related worsening) to known GERD presentations.
4. **Redacted Information:** Several pieces of information are redacted with asterisks (`*********`), including the exact time of symptom onset, duration, part of the past medical history, and one denied symptom. This indicates the diagram is based on a real but anonymized case.
### Interpretation
This diagram serves as a clinical reasoning tool, demonstrating how a physician synthesizes subjective patient history, objective test results (some of which may be conflicting), and established medical knowledge to arrive at a diagnosis.
* **What the Data Suggests:** The patient's presentation is classic for GERD: burning chest pain with specific triggers. While the endoscopic findings are somewhat ambiguous (erosions noted but later described as normal mucosa), the **pathophysiological evidence is conclusive**. The elevated Acid Exposure Time (AET) of 5.5% is a direct measurement of pathological acid reflux, which is the defining characteristic of GERD. This objective metric overrides the ambiguity of the visual endoscopic findings.
* **Relationship Between Elements:** The "Rationale" section acts as the critical interpretive layer. It doesn't just list facts; it explains *why* each fact is relevant to the GERD hypothesis. It bridges the gap between raw data (e.g., "AET 5.5%") and clinical meaning ("supports the diagnosis").
* **Notable Anomalies/Patterns:** The primary anomaly is the discrepancy between the initial endoscopy report (noting erosions) and the formal EGD result (normal mucosa). The diagram's rationale correctly identifies this as a common scenario where symptoms (NERD) can exist without visible damage. The pattern shown is one of **convergent evidence**: multiple independent data points (symptoms, endoscopic findings, pH monitoring) all point toward the same diagnosis, despite minor inconsistencies. The final diagnosis of GERD is therefore robust.
DECODING INTELLIGENCE...