## Diagnostic and Knowledge Data Structure
### Overview
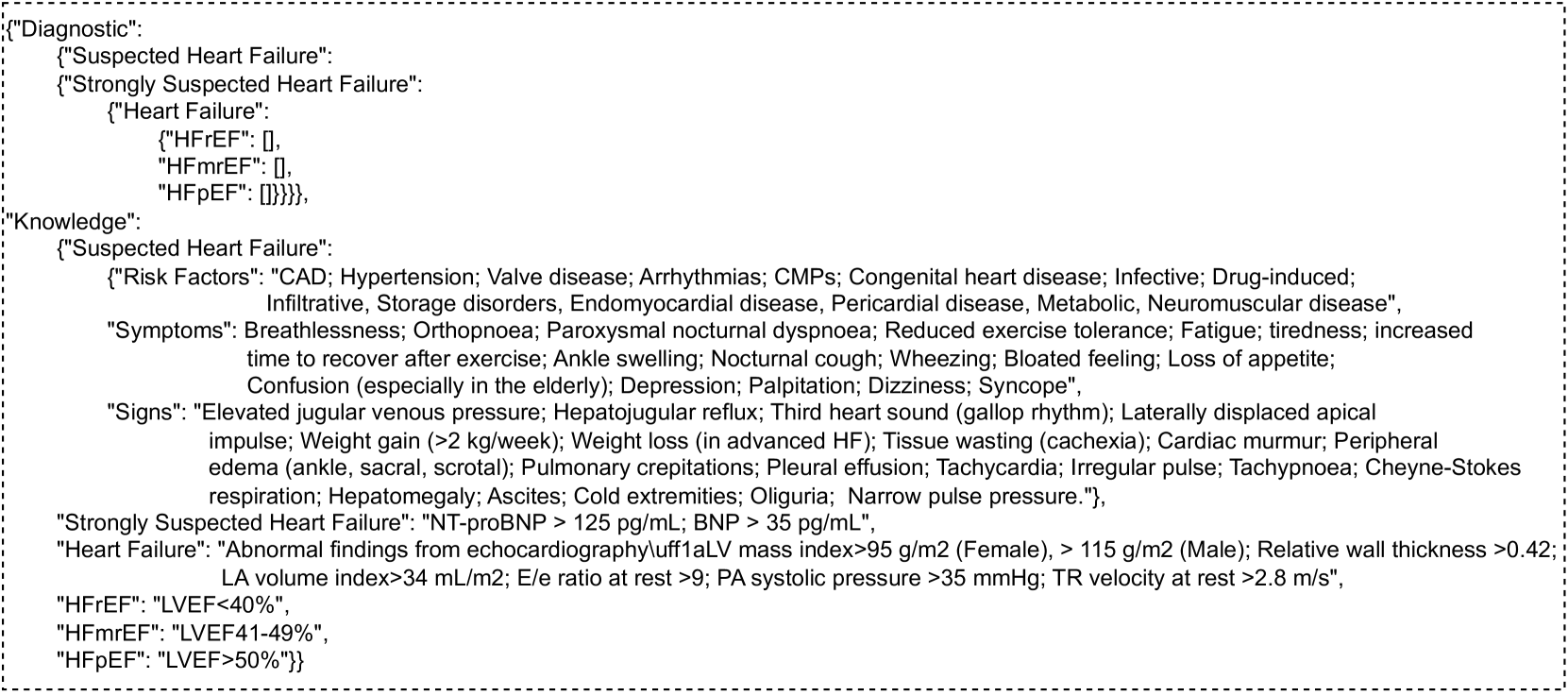
The image presents a structured data representation, likely in JSON format, containing diagnostic criteria and knowledge related to "Suspected Heart Failure." It outlines risk factors, symptoms, signs, and specific diagnostic thresholds for different types of heart failure.
### Components/Axes
The data is organized into two main sections: "Diagnostic" and "Knowledge."
* **Diagnostic**: Contains nested categories for "Suspected Heart Failure," "Strongly Suspected Heart Failure," and "Heart Failure." The "Heart Failure" category further breaks down into "HFrEF," "HFmrEF," and "HFpEF."
* **Knowledge**: Contains information about "Suspected Heart Failure," including "Risk Factors," "Symptoms," and "Signs." It also includes criteria for "Strongly Suspected Heart Failure" and "Heart Failure," as well as definitions for "HFrEF," "HFmrEF," and "HFpEF."
### Detailed Analysis or Content Details
**Diagnostic Section:**
* **Suspected Heart Failure**:
* **Strongly Suspected Heart Failure**:
* **Heart Failure**:
* **HFrEF**: Empty list `[]`
* **HFmrEF**: Empty list `[]`
* **HFpEF**: Empty list `[]`
**Knowledge Section:**
* **Suspected Heart Failure**:
* **Risk Factors**: "CAD; Hypertension; Valve disease; Arrhythmias; CMPs; Congenital heart disease; Infective; Drug-induced; Infiltrative, Storage disorders, Endomyocardial disease, Pericardial disease, Metabolic, Neuromuscular disease"
* **Symptoms**: "Breathlessness; Orthopnoea; Paroxysmal nocturnal dyspnoea; Reduced exercise tolerance; Fatigue; tiredness; increased time to recover after exercise; Ankle swelling; Nocturnal cough; Wheezing; Bloated feeling; Loss of appetite; Confusion (especially in the elderly); Depression; Palpitation; Dizziness; Syncope"
* **Signs**: "Elevated jugular venous pressure; Hepatojugular reflux; Third heart sound (gallop rhythm); Laterally displaced apical impulse; Weight gain (>2 kg/week); Weight loss (in advanced HF); Tissue wasting (cachexia); Cardiac murmur; Peripheral edema (ankle, sacral, scrotal); Pulmonary crepitations; Pleural effusion; Tachycardia; Irregular pulse; Tachypnoea; Cheyne-Stokes respiration; Hepatomegaly; Ascites; Cold extremities; Oliguria; Narrow pulse pressure."
* **Strongly Suspected Heart Failure**: "NT-proBNP > 125 pg/mL; BNP > 35 pg/mL"
* **Heart Failure**: "Abnormal findings from echocardiography\uff1aLV mass index>95 g/m2 (Female), > 115 g/m2 (Male); Relative wall thickness >0.42; LA volume index>34 mL/m2; E/e ratio at rest >9; PA systolic pressure >35 mmHg; TR velocity at rest >2.8 m/s"
* **HFrEF**: "LVEF<40%"
* **HFmrEF**: "LVEF41-49%"
* **HFpEF**: "LVEF>50%"
### Key Observations
* The "Diagnostic" section provides a hierarchical structure for classifying heart failure, but the lists for HFrEF, HFmrEF, and HFpEF are currently empty.
* The "Knowledge" section offers a comprehensive list of risk factors, symptoms, and signs associated with suspected heart failure.
* Specific diagnostic criteria are provided for "Strongly Suspected Heart Failure" based on NT-proBNP and BNP levels.
* Echocardiographic findings are used to define "Heart Failure," including LV mass index, relative wall thickness, LA volume index, E/e ratio, PA systolic pressure, and TR velocity.
* The definitions for HFrEF, HFmrEF, and HFpEF are based on Left Ventricular Ejection Fraction (LVEF) percentages.
### Interpretation
The data structure appears to be designed for a clinical decision support system or a knowledge base related to heart failure diagnosis and management. The "Diagnostic" section likely serves as a framework for classifying patients based on diagnostic findings, while the "Knowledge" section provides the clinical context and criteria for making those classifications. The empty lists under HFrEF, HFmrEF, and HFpEF in the "Diagnostic" section suggest that this part of the structure is intended to hold specific patient data or further sub-classifications that are not yet populated in this example. The provided criteria for "Strongly Suspected Heart Failure" and "Heart Failure" offer clear thresholds for objective markers, aiding in the diagnostic process.